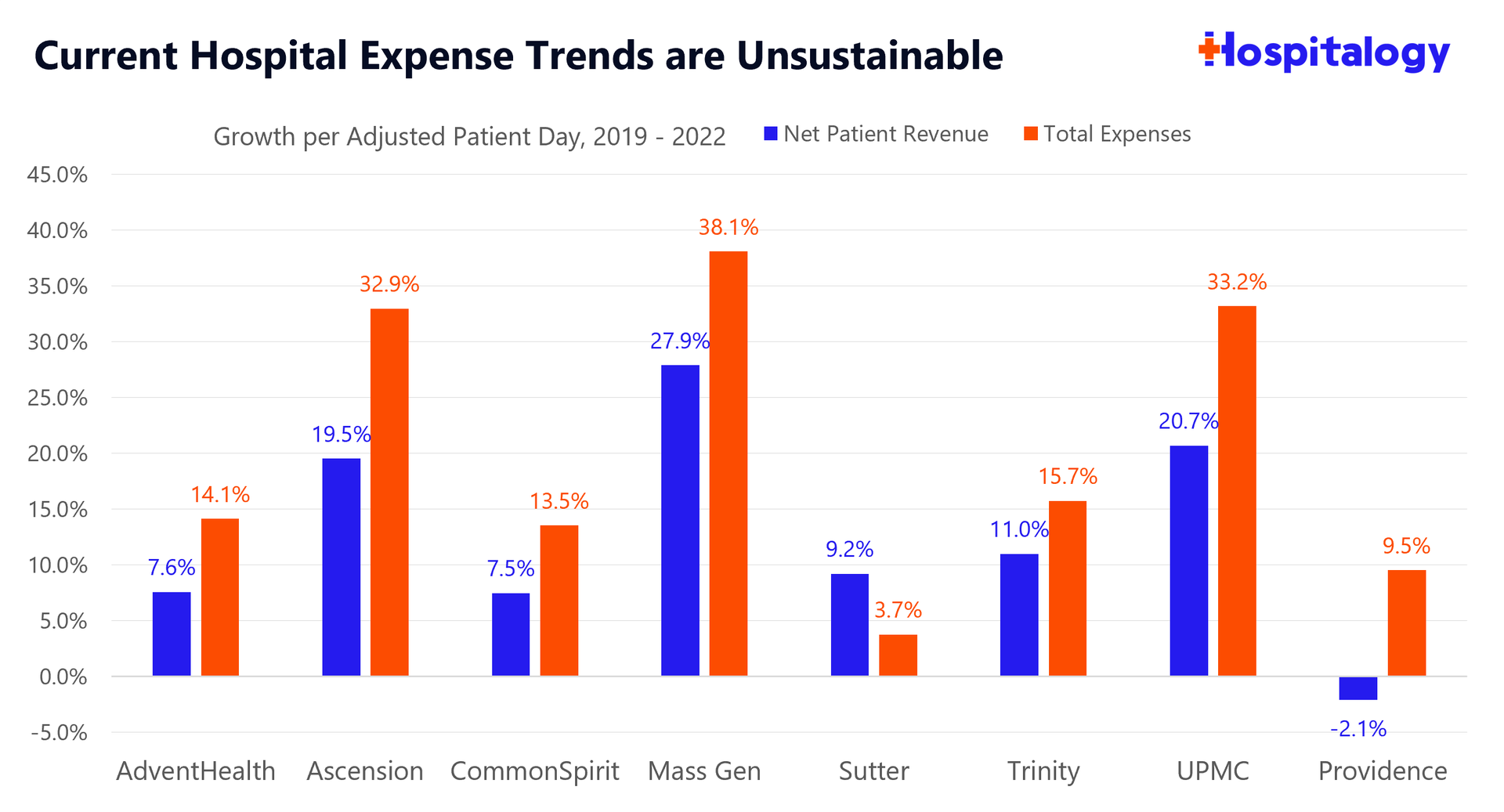
Source: Hospital EMMA disclosures, audited financial statements
When you take a look under the hood, the simple fact is that for the hospitals analyzed, operating expenses on the unit level are rising faster than revenues. For now, this trend is unsustainable and labor is where the number 1A focus is in C-suite hospital board rooms across the country.
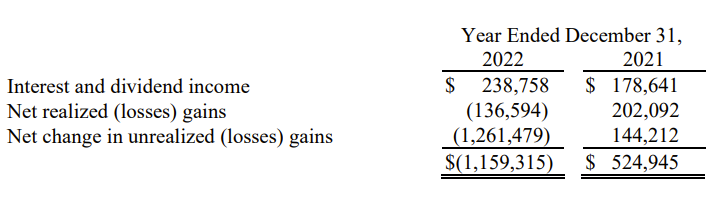
And that's the main problem at health systems right now. It's more than just the investment losses. That argument detracts from the more pressing issue affecting hospitals across the country. These health systems, in an ironically similar fashion to startups, are trying to find ways to cut costs, retain clinicians, and boost revenues in any way they can.
So…what happens when your core business expenses are rising faster than your revenues?
You get squeezed on margin and in the case of hospitals, have to shut down inpatient service lines, or outsource your revenue cycle management to someone like Optum, or lay off an increasing number of non-core personnel (e.g., the Novant innovation team RIP). All of which we've seen happen in recent memory.
Why do you think we're seeing these funky cross-market mega mergers or shutting down their existing joint operating companies (Centura, Amita, MercyOne)? The institution of the hospital is slowly crumbling, and chinks in the armor are forming. There's no more low-hanging fruit. Payors and CMS will only budge so much on reimbursement, and for now, what's left is the nitty gritty operating stuff that needs to get optimized.
When will things improve? As the labor market settles down and the nursing supply increases, volume will continue to return. Health systems will likely secure higher commercial reimbursement from payors over the next 2-3 years. Things may settle, and everything will be peachy if the AHA gets exactly what it wants…
..But these dynamics don't address the more secular problems facing hospitals - E.g., the shift to Medicare (& Medicare Advantage), policy shifts aimed at reducing ED visits and admissions, and the general shift to outpatient as innovators optimize surgery and patient care delivery outside of the hospital.
Parting Thoughts: Let's compromise.
While the criticism surrounding hospital investments and operating as de-facto hedge funds is credible, there are bigger fish to fry. There's a disconnect between the arguments, and a disconnect in general in healthcare.
Do hospitals deserve constant financial support and policy babying? That's an argument for another day, and a nuanced discussion - but that money could be used elsewhere in payment policy supporting a wide range of services.
It gets tricky, because hospitals hold a ton of inefficiencies and admin bloat, yet they support jobs in local markets. They also provide care for local communities, and patient like them as I mentioned in my MedPAC analysis. Finally, portfolios are used to invest in economic development and innovation (despite the hedge fund criticism).
In general, hospitals are described as the 'department stores' or 'all you can eat buffets' of healthcare, and it's hard to be an efficient operator when you do everything and are burdened by a ton of regulation or dumb governance structures that slow down everything known to mankind.
What do we want the end game to be for hospitals, with rising expenses and low political sympathy/appetite for support? I'm not a policy expert, but some fodder for discussion:
- If you think hospitals should exist in the current status quo, then you should join the calls for increased government funding, higher payor reimbursement and support for hospital based care.
- On the other hand, if you think other care delivery models deserve to be supported amidst the secular shift to Medicare and outpatient care, then you should be asking hospitals to lean up, cut down on admin bloat, reign in executive pay, and focus on retaining & support of clinicians.
Me? I'm in the middle of the aisle. Let's allow hospitals to evolve but also support that evolution. To do what they do best in caring for high acuity patients and extreme situations. Then let's partner and work together on the other stuff, to deliver better patient care in better settings with less bureaucratic crap, prevent exploitation of policy, and reign in practices that burn out clinicians.
Hospitals will have to want to evolve, though. And that evolution will be painful.






No comments