Telehealth Exclusive: What works for telehealth post pandemic boom
Doximity
It's been a few years since we saw the mad scramble among providers to move appointments virtual, and now we're beginning to see what use cases might stick around for the long haul. In its 2023 State of Telehealth report, the "LinkedIn for doctors" site and telehealth platform Doximity offers insights on what providers think their patients need from virtual care today — starting with an easy-to-use site and the ability to add family members to the call.
Doximity, which went public in 2021, lets individual providers use its site for appointments for free; health systems pay a licensing fee for additional features like EHR integration. The report is compiled from surveys of 1,200 clinicians and 2,400 patients across the country.
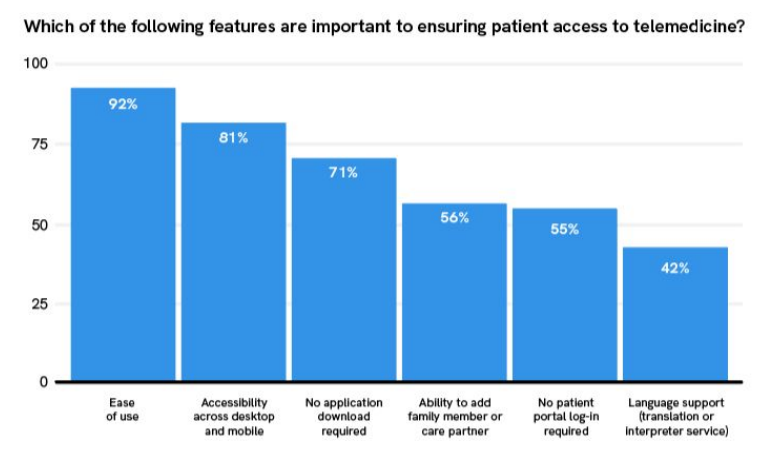
About 92% of doctors said "ease of use" was key to ensuring patients could access virtual care. Other factors that help include not requiring users to log into another patient portal, language support, and no additional software downloads.
Co-founder and chief strategy officer Nate Gross told STAT's Mohana Ravindranath that providers and patients used the telehealth site more after Doximity built in a feature to add family members. They also liked a feature allowing doctors to send post-call follow up notes directly to patients' phones, which could then be forwarded to family caregivers. A feature alerting doctors and patients to poor internet connections served as gentle encouragement to move to a better spot.
"Being able to passively nudge leads to less animosity and frustration on calls," he said.
Medical Devices
Industry criticizes EPA rule limiting ethylene oxide
In April, the Environmental Protection Agency proposed new limits on the use of a carcinogenic gas called ethylene oxide. While that might seem uncontroversial at first glance, ethylene oxide is currently the only way to sterilize medical devices that can't be exposed to steam, including pacemakers, catheters, and ventilators. In public comments on the rule posted this week by lobbying groups, manufacturers expressed concerns that the EPA's crackdown would lead to device shortages. AdvaMed estimated that the ethylene oxide limits would bring facility capacity to sterilize devices down by 30 to 50%.
Mark Leahey, head of the Medical Device Manufacturers Association, argued the combined proposals "would be devastating for patient access, and as FDA noted after the EPA began to look into this issue, without an adequate availability of EtO as a sterilization method, the impact to patient care would be catastrophic."
But the long-term risks of exposure to ethylene oxide are clear, particularly for communities living near sterilization plants, which are often disproportionately low-income or of color. EPA's primary goal with the rule is to decrease the number of people living with 6 miles of a plant by 96%. Several commenters, like the Alliance of Nurses for Healthy Environments and the National Tribal Air Association, commended the EPA rule and advocated for stronger measures.
Health equity
Medical experts explore how to eliminate bias in clinical algorithms
Racial bias is baked into technologies used across medical practice, but at a conference on the topic hosted by the Doris Duke Foundation this week, experts were divided on what exactly to do about it. For all the problems it creates, some doctors argue that simply pulling race out of clinical calculators and algorithms without a suitable physiological replacement could "do more harm than good."
At the conference, the foundation announced $10 million in grants meant to aid organizations in revamping their processes. One notable effort highlighted by STAT's Lizzy Lawrence and Katie Palmer is a project that aims to test a replacement for the American Academy of Pediatrics' 2011 guidelines for diagnosing urinary tract infections in children up to age 2. The algorithm took into account if a child is black or white, which "skews the workup," the academy's chief health equity officer Joseph Wright said on a press call ahead of the event.
"Race is not a biologic proxy," said Wright. "Race is a social construct and has no place being embedded in a clinical guideline like this."
Read more here.





No comments