Happy Wednesday , Hospitalogists! Here's part 2 of my talk with Pete McCanna, CEO of Baylor Scott & White. Part 1 was all about Baylor's consumer-centric strategy, and today's edition will cover all things health system economics—discussing physician alignment, provider-sponsored plans, local market dynamics in Texas (and why nuances between markets matter), and Pete's thoughts on AI in healthcare. Lots of great stuff in here.
Let's dive in! And please share your thoughts with me. I got a great reception on part 1, so I hope you enjoy part 2 as well. Part 3 on leadership will be Thursday, and this whole series will be posted on the Hospitalogy site then as well. |
Was this email forwarded to you? |
|
|
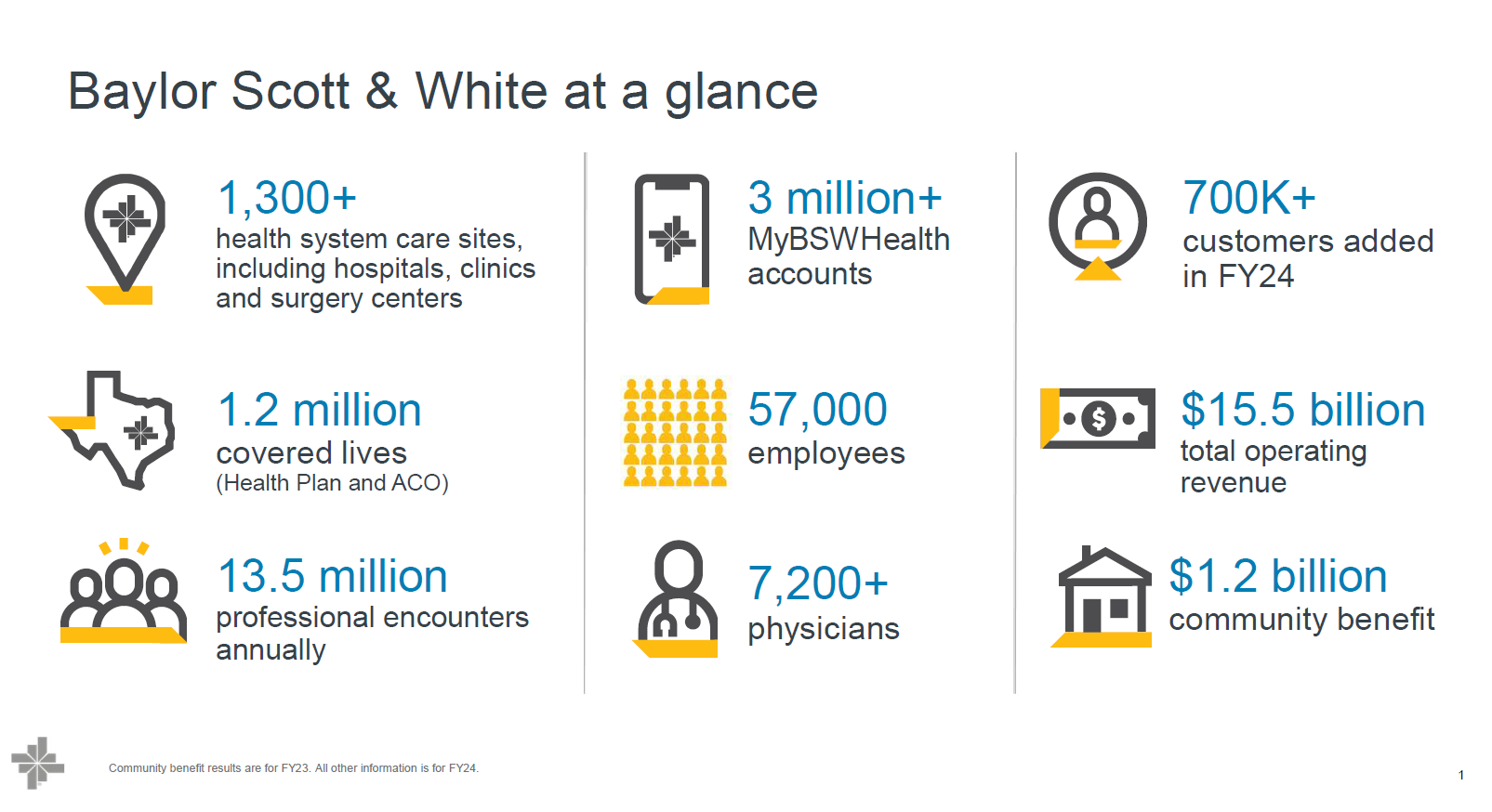
The Baylor Breakdown: Part 2 |
Baylor's Physician Strategy with HTPN |
A more nuanced line of questioning I asked Pete related to Baylor's physician alignment strategy—specifically, what's going on in Baylor's markets, his thoughts on the current state of the subsidy model (which has been characterized as unsustainable), and which approaches work in which market. Here were some takeaways: Every market is different for a health system, and different tactics are needed in each. However, there's one constant: you need to have a critical mass of physicians—a comprehensive, employed medical group with strong specialty coverage. And if you operate a fully integrated platform, you can—and should—also include independent physicians within that network. Having this asset is vital for several reasons: - Baylor can credibly deliver on a risk-based relationship with an employer or payor and bring the full continuum of care—with uniform standards within Baylor's ecosystem—without relying on anyone else.
- The physician or professional entity serves as an innovation center: a place where Baylor can launch new products and services, refine and iterate on them, and then scale them to the rest of the enterprise once perfected. Often, the employed physician base leads health system innovation. Having that capability within Baylor's employed group is important.
- The organization acts as a training ground for great leadership, in the long term. Many senior physician leaders at Baylor have risen through the employed group and distinguished themselves. In Baylor's model, physician leaders eventually reach a point where they run a sector of the business. Pete specifically mentioned a surgeon in Austin who is now the EVP helping to run the entire delivery system in Baylor's dyad leadership model.
|
Physician Employment and Subsidy Model – What's the Outlook, and Is It Sustainable? |
Ultimately, whether your physician alignment model works comes down to where the value creation lies. Ask yourself: what's the job to be done? For instance, acquisitions and consolidation of physician practices make sense if you can draw a clear line to the patient and demonstrate how you improve patient care. They generally don't work long term if you're engaging in financial engineering or arbitrage, which is why we saw some of the PPMs falter over the past few years. With the various physician employment models, the biggest question is…what KIND of value are you creating? And why is that health system—or PE or other consolidator—employing physicians? Is it to arbitrage rates? That type of financial engineering and 'non-value' creation is going to disappear. The question is whether there are employment models that lead to genuine value for the customer and whether those models are economically feasible. Take risk management as an example. If you can create a model of care through a tighter relationship—for instance, using senior-only clinics—patients generally appreciate it. They're getting more access; some even receive 12 or more touchpoints per year. DTC specialty care is a new trend. It's unstoppable. In certain conditions, consumers will be armed with enough knowledge about their own conditions—using AI and similar tools—so that they want to go straight to the specialist. |
Provider-Sponsored Plans: What Do These Unlock for Baylor, and Are They Viable? |
Notably, provider-sponsored plans scaled back from Medicare Advantage (MA) in 2025 and lost considerable market share. For Baylor, however, Pete mentioned a couple of key roles these plans play as part of an overall enterprise strategy. In certain markets (e.g., central Texas), having an insurance entity that collects premiums provides a model that helps Baylor operate a closed-loop system—especially in government segments (Medicare, Medicaid). This is a perfect example of why local market differences matter. For instance, demographically, the population in central Texas sees less turnover. On the Medicare Advantage side, when Baylor holds a critical mass of providers in a certain geography, they can launch an MA plan in lieu of working with carriers. Finally, for self-employed large employers—working in conjunction with Baylor's ACO, Health Plan, and app—Baylor can customize an array of products and services catered to employers. Baylor offers a portfolio of solutions that covers all the major needs of these organizations, all integrated into an app, giving Baylor the ability to assume employer risk. At a high level, although it's not exactly a money-printing machine, the risk-based part of Baylor's business supports the overall, system-wide strategy. Increasingly (and notably), Baylor believes its health plan needs to become a platform experience as well, and the advantage is that they can control that trajectory. In general, healthcare is moving toward platforms over time. Pete's final strong point on provider-sponsored plans centered around the challenges they face against savvy competitors. By definition, provider-sponsored plans are subscale. This regional dynamic means that larger national plans will always be more efficient than you. So the question is…how can you create scale—not only in density but also in capability through AI, data, and other necessary components for managing risk? The answer is…through collaboration. To that end, Baylor is working with Longitude Health to develop a population health platform. This nationally scaled solution can then be sold to subscale plans to share the benefits of scale without needing to be a national player. An interesting, notable little venture. |
Local Market Dynamics Matter |
One more note on the power of local market dynamics to drive the point home:
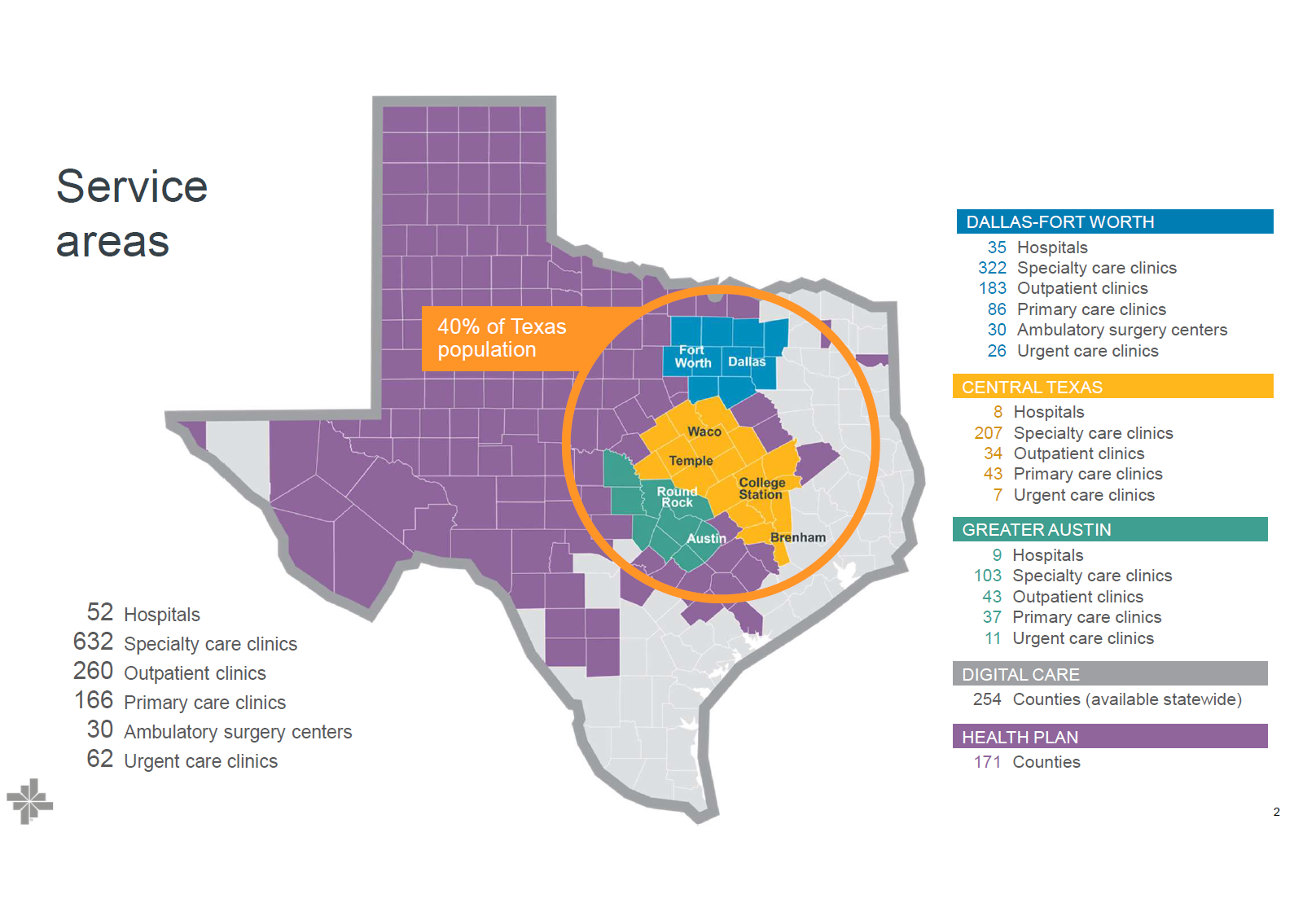
Baylor's markets have nuances that affect its strategy in each particular area. While Baylor's overall enterprise strategy and core customer-centric theme remain the same, each market requires different tactics to achieve the best results. For example, Austin is distinct from Temple or College Station. In Austin, while Baylor might not be the largest player by market share, the organization holds the largest employed physician group in the city. With that crucial asset, Baylor is carving out a niche with more flexibility and nimbleness than, say, HCA or Ascension. Even as they build out their Austin presence, the shift toward health system transformation (rather than old-school tactics) is clear, and their integrated offering will grow over time.
Moving to Central Texas and Temple, Baylor holds a 75% market share, and there's much more government reimbursement, so taking on Medicaid or Medicare risk makes sense—they dominate these areas.
Finally, in DFW (!!), health plans don't play as significant a role, but ACOs take precedence. Physician dynamics in DFW lean more toward independent private practices. According to Pete, half of DFW physicians are either in private practice or not affiliated with a health system, making tight integration in Dallas more challenging. On the commercial side, DFW is an open-choice market, so taking on commercial risk isn't as viable.
These are just a few examples of market nuances in Texas alone. Now, imagine scaling that to hundreds of MSAs across the country, across health systems, payors, and every healthcare services organization in between!! |
Baylor and Innovation in AI |
Of course, I had to ask Pete about AI in healthcare and how he sees Baylor leveraging it across the organization. Baylor is a big believer in AI—but the big question is "how do you adopt it?" Pete described AI as akin to throwing rocket fuel on their customer-centric approach because AI is at ALL of our fingertips, equipping patients with more knowledge. For instance, during a sprint review, Baylor identified a pain point: people get their lab results but don't know what they mean, so they have to wait for the doctor. Now, patients can upload lab results to an AI system (with de-identified data fed into an LLM) to get an extensive evaluation of possible explanations for abnormal values. AI also turbocharges Baylor's virtual tools and further empowers patients. Today, patients have access to much more information than they did even five years ago. I can personally attest to these capabilities. When my son had some gut issues, I uploaded his results to ChatGPT and was able to understand what all the various bacteria levels meant. Pretty cool—and very empowering from a consumer perspective. On the flip side, as an administrator or physician, you must assume that every patient you meet may have already run their symptoms or lab results through ChatGPT. This dynamic is entirely new and demands better communication with patients to maintain trust. The scope of healthcare is so vast because of its labor-intensive nature, and AI will eventually be infused into everything in the field. As with other product developments, Baylor is assessing every area and asking, "What's the application of AI in this environment?" In 2024, Pete met with OpenAI and several other health system and payor executives, and he was stunned by some of AI's capabilities—such as differential diagnosis—so he's excited for the future on both the administrative and clinical sides. He even thinks AI will totally change primary care; the PCP will oversee AI and care teams over a much larger panel of patients, helping bolster access. That's pretty cool. Pete broke down AI solutions into three buckets: Individual use cases. In a protected enterprise environment, can Baylor provide you with your own personal assistant to use within certain parameters? For example, it can help with marketing press releases, legal drafts, or personal workflows. You can generate these outputs almost instantly rather than waiting for someone to type up a template. (I use it for that purpose too—even though it STILL sometimes hallucinates…sigh.) New and existing cases of AI. - We're seeing a revamp of legacy systems that are now infused with AI. For instance, in imaging: if a radiologist is working through his queue and someone enters the ED, AI can read the image before the radiologist does, triage certain images by flagging potential critical findings, and alert the doctor to stop the queue and review a critical image. With a smart system handling triage, the process is much faster and significantly impacts patient outcomes and ED throughput.
- In Pete's view, it'll be malpractice NOT to use AI-assisted tools because they'll be that effective. I share this viewpoint. While many focus on the safety, compliance, and responsibility of AI—what I liken to the 'self-driving car' problem in healthcare (self-driving cars are statistically safer than human drivers, yet every crash makes headlines)—guardrails are important, but we should be pushing AI forward as much as possible, responsibly.
AI-native solutions: Pete specifically highlighted AI's translation capabilities (given that health systems spend millions on translation systems) along with agentic AI performing redundant tasks in areas like HR benefits, legal, and patient intake. For example, AI can listen to thousands of conversations to identify common issues and solve patient problems without direct human intervention—the list goes on. Co-development. Baylor is developing new products (such as navigation tools) and is open to partnering with outside companies to infuse these products with an AI-enabled feature set. The biggest force in AI and innovation right now is the velocity of change. Technological improvements are occurring so quickly that major changes can be seen every 60–90 days, which keeps upping the stakes for everyone involved (and even significantly affects the pricing of AI solutions). It's exciting to see it all unfold in real time. |
|
|
SPONSORED BY THE GARAGE Some of the best companies in healthcare don't chase the spotlight; they chase results. And one of those companies is The Garage. Since 2012, they've quietly built a powerhouse platform that supports 140+ ACOs and touches 15M+ lives.
From data ingestion and care coordination to risk adjustment and AI copilots (yes, plural), Bridge isn't just a dashboard.
Pop health folks already know. But as for everyone else, this is what effective healthcare innovation looks like. I just dropped a new deep dive on how they're doing it.
Check it out 👇
|
|
|
Random personal anecdotes and musings from me |
Alright, I know you all came to this section expecting all of my Masters takes so here we go: - Probably the best Masters since 2019, and a top 3 Masters in general (at least in my lifetime). The storylines were all there with Rory chasing the green jacket and his grand slam. The only part that stunk was that Patrick Reed was anywhere close to the top of the leaderboard. Someone really shoulda taken one for the team there
- Gotta feel for Justin Rose. Absolute warrior and such a consistently good golfer and great guy all around. He handled the post-round interview with such class. You can't not root for him, and he always seems to hang around in majors. I wouldn't be surprised to see him scrape out a W before he's down and out.
- Rory...my guy...you are the most talented golfer in the world and you were on full tilt for half of the round. The fact that he overcame four double bogeys (maybe even five?) to win means he had to make 20 birdies!! I couldn't believe my eyes. To see one of the best golfers in the world miss a 100 yard flip wedge abysmally into the water on an easy par 5, then pull off a swinging, rising, swooping high draw around a tree 210 yards to 5 feet is the most unreal volatility and unhinged behavior I've seen on the course. I cannot believe he still won after missing that first putt on 18. But hey, credit to the guy for putting together 3 magnificent shots in the playoff. If that putt had been a foot longer to win it, I'm convinced he would have missed.
- I miss vintage Spieth
- Bryson is fun to watch but his swing and distance control was all over the place. I really think the course affects his game more than he lets on. Mr. trigonometry over there can't figure out those ski slopes.
|
|
|
Thanks for the read! Let me know what you thought by replying back to this email. — Blake |
|
|
.png) | Share Hospitalogy, Earn Rewards | Have friends who'd love Hospitalogy too? Click the link below to share Hospitalogy with your friends and earn awesome rewards! | |
|
PS: You have referred 0 people so far | | Share Hospitalogy! | |
|
|
|
|
Get your brand in front of 43,000 executives and healthcare decision-makers. |
I'm building an exclusive community for professionals working on health system transformation. |
Workweek Media Inc.
1023 Springdale Road, STE 9E
Austin, TX 78721 Want to ruin my day? Unsubscribe. |
|
|
|






No comments