Happy Wednesday, Hospitalogists! Value-based care (VBC) sounds elegant on a slide. Shared savings…shared risk…shared purpose. Payors and providers working in lockstep to achieve the triple…er…quadrupl….uhh…quintuple aim. But this massive healthcare paradigm shift has been lost in the maze of administrative headache. In reality, VBC today looks more like a spreadsheet labyrinth. Manual Microsoft Excel workbooks run value-based care, not sophisticated datasets or intelligent insights with next best action (as an Excel fanboy, this hurts to say). - Providers spend months negotiating what should be an alignment exercise in a contract, then spend the rest of the year trying to figure out whether they are winning or losing the deal. Payors push giant claims files over the fence and dust off their hands.
- Clinical teams do the right thing for patients, then discover six months later that cost trends went sideways and the contract is underwater, leading to frustration.
- Actuaries trying to determine risk and forecasting, pull incongruent datasets that barely give them access into their organizations' performance market by market, peeling back the layers like an onion.
In fact, the whole of value-based care can be described as an onion: layers upon layers of complexity and siloes, when really all you need is a sharp knife to come along and cut through the noise. Arbital Health is that knife slicing through the VBC onion. They're the infrastructure layer VBC so desperately needs. So I'm here today to tell you more about them, and how they're tackling big hairy problems in risk-based contracting and more. |
This essay is a sponsored post in partnership with Arbital Health. I write these posts for companies with products or missions I believe can provide value-adds for Hospitalogy subscribers, many of whom work with/for ACOs, integrated health systems, health plans, and other risk-bearing organizations that want to learn more about potential value-based care partners. If you're interested in a sponsored deep dive, please reach out to blake@workweek.com! |
|
|
Key takeaways to know about Arbital Health |
- From an ROI and value-add perspective, Arbital's message to payors, providers, point solution vendors, and VBC enablement firms is…it's time to scale VBC, and we can help you with that. Go from two risk deals to five, or from five to fifteen, without hiring a platoon of analysts and actuaries to rebuild manual logic every time. And Arbital holds the platform to make it all happen.
- Arbital enables risk-bearing orgs to manage risk contracts at scale, to more rapidly drill down into populations program performance, disease states, utilization metrics, and financial results across an entire at-risk population.
- Their team's platform digitizes high-volume of contract logic, ingests medical, pharmacy claims, eligibility, and revenue files, runs continuous performance measurement, and reconciles the contract performance with audit trails.
- Arbital's Contract Intelligent AI agent reads dense agreements, answers contract questions, and powers self service analysis across populations, markets, and measurement periods. AI accelerates actuaries with faster, deeper insights so they can work at the top of their game.
- Proprietary benchmarking and digital twin matching reveal where cost is off trend in near-real time rather than months-long lags, then point to the cohorts and services driving variance to prioritize for member interventions.
- Arbital's data views unify financial and clinical leader decision making - so everyone is finally working from the same data set and not manual, disparate spreadsheets. The CFO's view ties directly to the CMO's view, which means decisions move faster and arguments fade…breaking down organizational siloes.
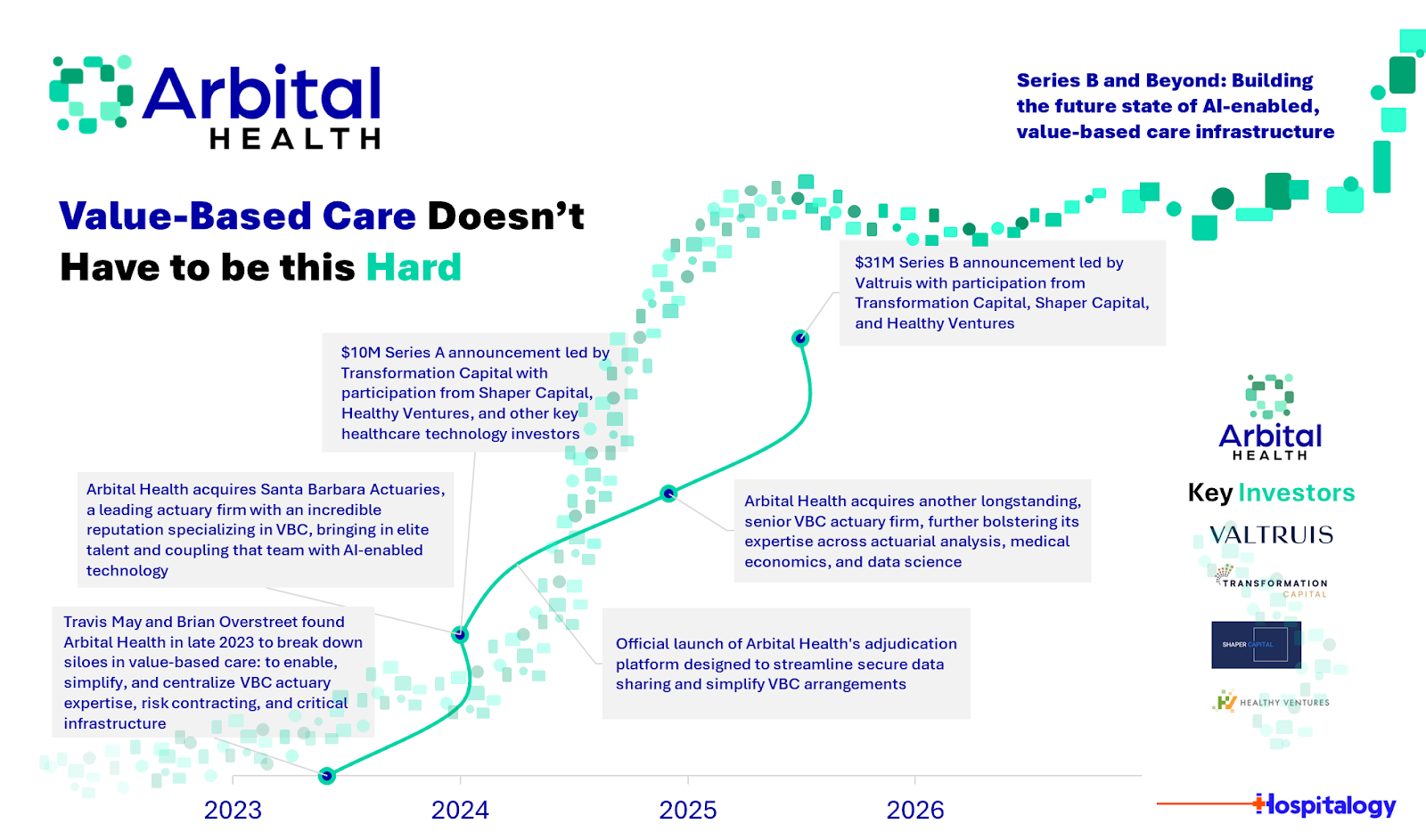
- Arbital also raised a $31M Series B, led by the fine folks over at Valtruis! Arbital already supports providers and enablement groups, and now they're looking to push upstream so health plans can operate portfolios of VBC deals on standardized rails.
- With this funding, Arbital will broaden its focus to support payors' toughest challenges with new capabilities, while continuing to empower providers expanding benchmarking capabilities for precise outcome measurement, strengthening forecasting to project year-end contract performance, launching a conversational actuarial agent that answers complex questions in seconds and activates Next Best Action + workflow automation to align stakeholders and drive VBC success.
CALL TO ACTION : Get in touch and learn more about the Arbital platform here. In my humble opinion, a must-take meeting for any risk-bearing org to make sure you're on top of your VBC infrastructure game. |
The problem Arbital is trying to solve and the current state of value-based care infrastructure |
In 2024, Arbital Health stepped into the fray with a simple thesis: Value-based care doesn't have to be this hard. What VBC needs is a simplified, streamlined operating infrastructure transforming the manual, brittle parts of risk contracting into a repeatable system. So Arbital honed the knife for the VBC onion. Arbital's platform provides the critical infrastructure to successfully manage risk-based contracts, a shared set of rails that payors, providers, and risk-bearing organizations can run on. It combines actuarial depth with modern software and applied AI so actuaries work at the top of their license and enables enterprises to get their siloed teams on the same page: clinical teams act on the same source of truth as finance, which has never (or rarely) happened before. When I chatted with the Arbital team about this piece, their leadership summarized the aim of the company directly in our conversation. Value-based care risk contract reconciliation has existed for a very long time, mostly on spreadsheets, with heavy manual lift and constant back and forth. Arbital's platform is built to change the mindset. It does not have to take that long. It does not have to be that painful. |
Arbital just closed a Series B. Investors leaned in because the boring plumbing of value-based care is where scale happens. The winners in this next phase will not be the loudest care navigators or the flashiest front doors. No - the winners will be the firms that make the money move correctly, transparently, and quickly across thousands of contracts and millions of patients. Arbital is building the future chassis of value-based care. The major barrier to continued VBC adoption is not belief. The barriers lie in operations. The day-to-day blocking and tackling: - Contracting takes too long.
- Every agreement is bespoke.
- Once live, the data lags and the math diverges.
- Payors and providers maintain separate spreadsheets with different baselines, different trend assumptions, and different attribution lists.
- Reconciliation becomes a negotiation rather than a measurement.
- By the time everyone agrees on what happened, the year has rolled over and the next contract starts with a trust deficit.
The burden concentrates on providers and risk bearing physician groups. Whether they're vertically aligned or collaborate hand-in-hand with a payor, or they're part of a hospital's ACO, or independent, all of these groups face similar challenges in risk. They receive a boatload of information like claims, eligibility extracts, and CMS revenue data and have to make sense of it all. A health system then pays for actuarial support just to discover basic facts like current medical loss ratio versus target or pharmacy PMPM in one region is blowing up the budget (maybe even a handful of patients or a specific disease category!). All of this work takes an excruciating amount of time. Analysts stitch together extracts from multiple payors, each with different service categories and different quality definitions. Nothing lines up. Clinical teams operate with population health reports that rarely tie cleanly to financial performance, so smart interventions do not reliably turn into savings. The VBC software stack reflects that fragmentation. Point solutions solve care gaps, referral leakage, or readmission risk. Few tools encode the full contract math, then tie it to performance and final settlement. So organizations end up with analytics on one side, contract terms on another, and actuarial models off to the side in a workbook that only two people understand. This state of VBC is not an infrastructure. This is more like a Swiss cheese industry with gaping holes to fill by humans, manually, time and time again. |
How Arbital solves that problem |
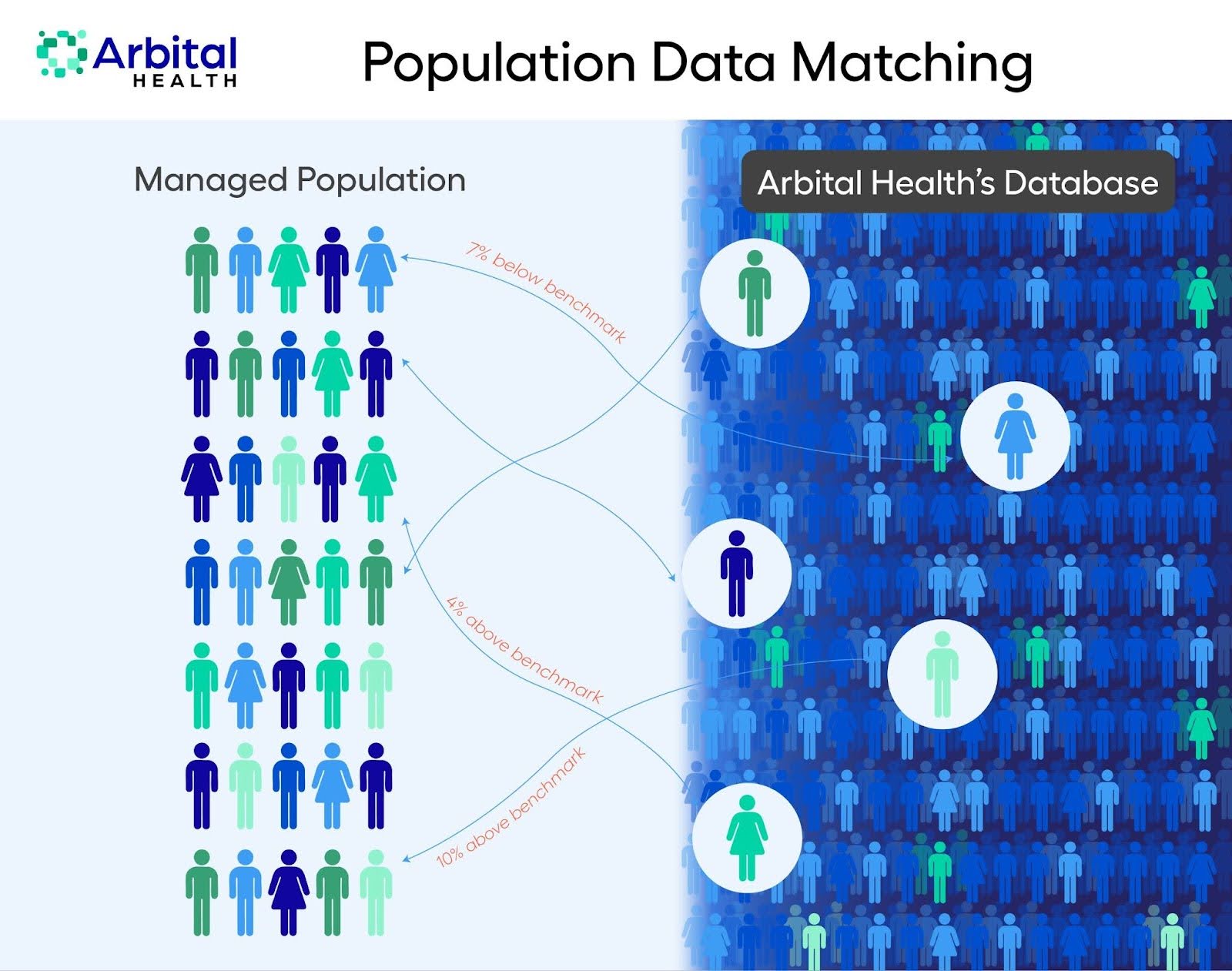
Arbital treats value-based contracts as software, not as one off projects. First, the company digitizes each and every agreement. The platform ingests long, legalistic contracts and extracts the parameters that drive the flow of incentives. Measurement periods, attribution rules, risk corridors, shared savings splits, stop loss, quality gates, pharmacy carve outs - and how those align with outcomes and ultimate money outflows. Second, Arbital normalizes the data. The platform connects to payor feeds for medical and pharmacy claims and eligibility. It runs enrichment and categorization using proprietary measurement libraries, which means a knee replacement, an infusion, and a brand specialty script all land in the right buckets the same way every time. Data quality checks fire early. The result is an analytics ready asset with consistent definitions across programs and markets. Third, Arbital measures continuously. Instead of waiting for quarter end, the platform tracks performance month by month and throws signals when spend goes off benchmark for a disease category, a site of care, or a geography. And here's an incredible piece of secret sauce Arbital that impressed the hell out of me: Arbital has trained a proprietary benchmarking database that matches actual patients within certain disease states to a digital 'twin' within the Arbital database. The digital twin benchmarking compares each managed member to a statistically similar counterpart from a de-identified reference set. For instance - if the diabetes population in Kentucky runs hotter than matched peers from the dataset, those working in the Arbital platform will see it now, not in six months (as we've seen lagging payor data crush risk players at times). |
Fourth, Arbital automatically reconciles contract performance. The actuarial module runs IBNR calculations and completion factors to provide an accurate view of the contract from the current claims run out and project final results before all claims have landed. It calculates MLR, shared savings, and settlements according to the digitized contract. Scenario tools let finance leaders adjust assumptions and see how actions would change the payout. That turns contract reconciliation into an operational cockpit rather than a retrospective book report. Finally, Arbital aligns the humans. Subtle, underrated, and often overlooked, especially in this context. Finance and clinical leaders log into the same system and view the same truth. - The CEO can see measurable change from engaged members.
- The CFO can see the dollars.
- The Chief Actuary can manage risk.
- The CMO can see the cohorts that move those dollars.
- Care teams act on live signals rather than waiting for requests from actuarial.
Everyone starts from the same baseline and the same measurement period definitions, which reduces the debates that slow down real work. For questions that teammates are too scared to ask each other or for information needed quickly, soon Arbital's AI agent is there to answer all sorts of easy or complicated questions alike - including PMPM targets, MLR thresholds, or the quality hurdle required before savings accrue. That gets every stakeholder on the same logical blueprint from day one. It's time to start thinking like an enterprise and less like a mutated amalgamation of moving parts, folks. And yes, I really just wanted to use the word amalgamation there. Enough semantics. What's the actual Arbital platform like? What would you be working with? Let's dive in. |
Product and platform rundown |
Arbital is a modular SaaS platform built for the full value-based contract lifecycle. The core pieces work together on a unified data model. |
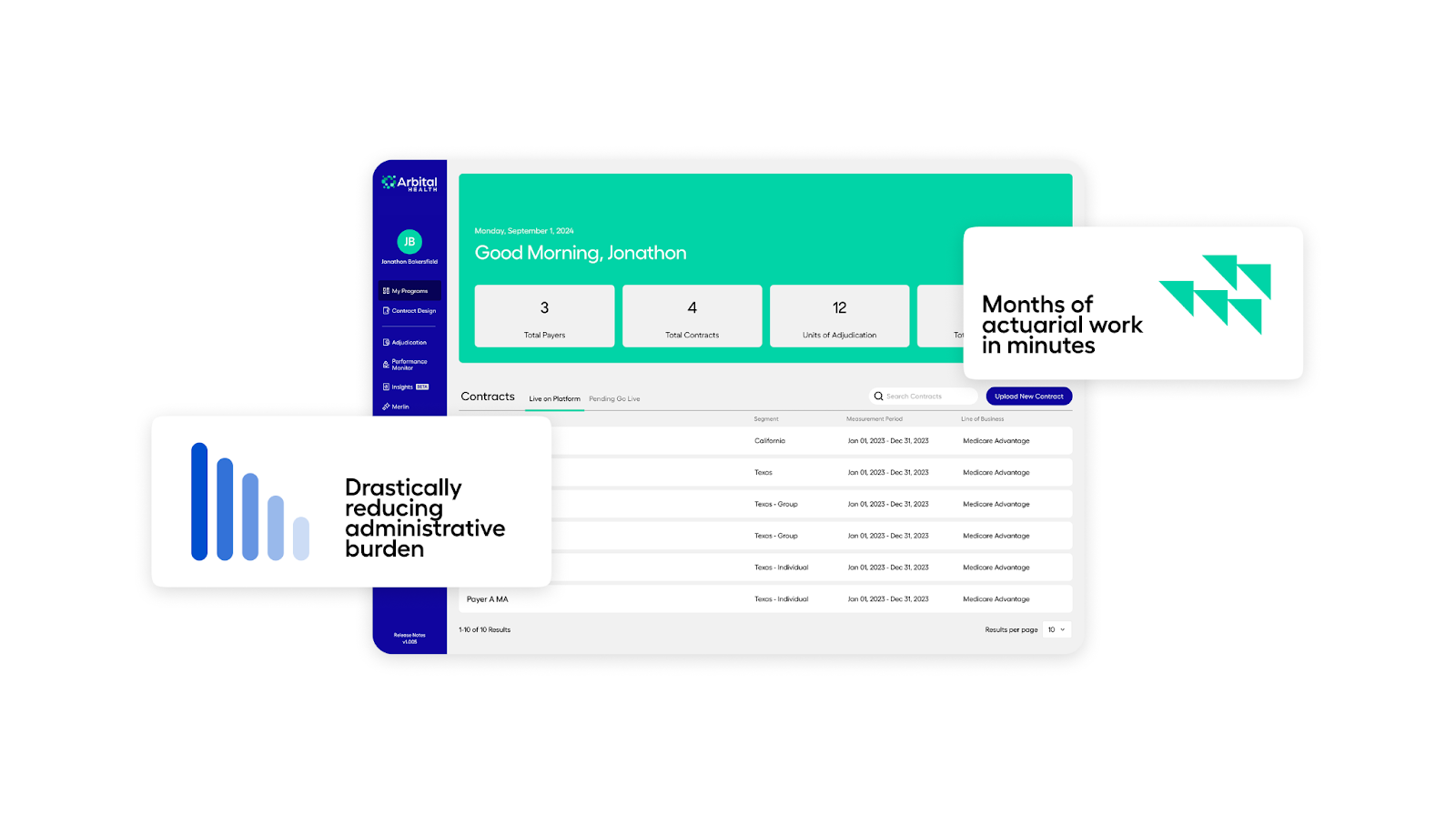
My Programs - The entry point to Arbital's platform. Contracts get ingested, parsed, and turned into structured logic. The Contract Intelligence AI assistant can answer contract questions and surface key terms without a manual hunt. Measurement periods are set, attribution logic is codified, and the platform is ready to accept data for those members.
Data Ingestion and Enrichment - Arbital ingests claims and eligibility feeds and runs them through proprietary measurement libraries. Services are mapped to consistent categories across payors and lines of business. Pharmacy and medical spend land in the right places, quality measures are aligned to contract definitions, and anomalies are flagged. The goal is the same vocabulary across every contract you manage.
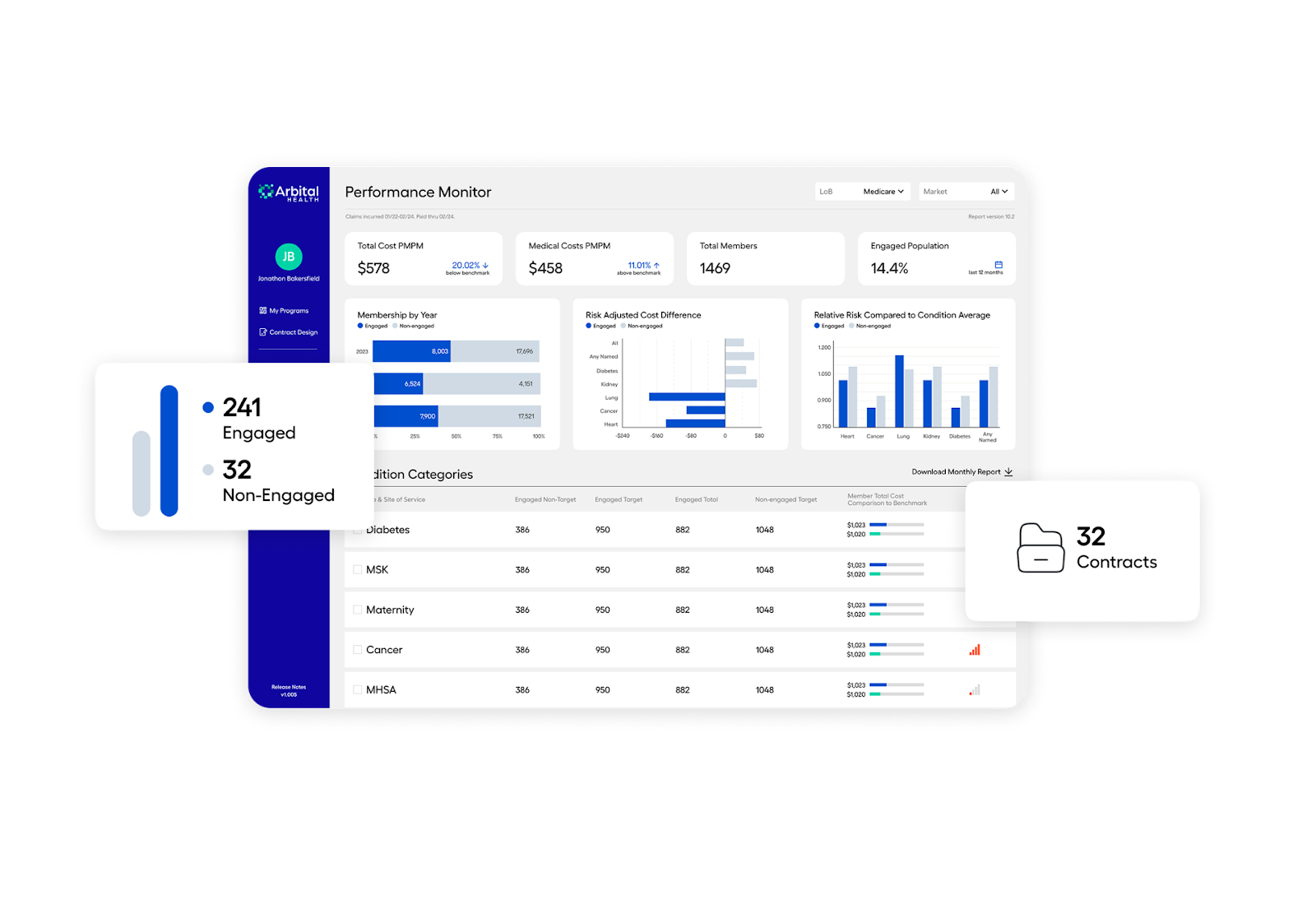
Performance Monitor |
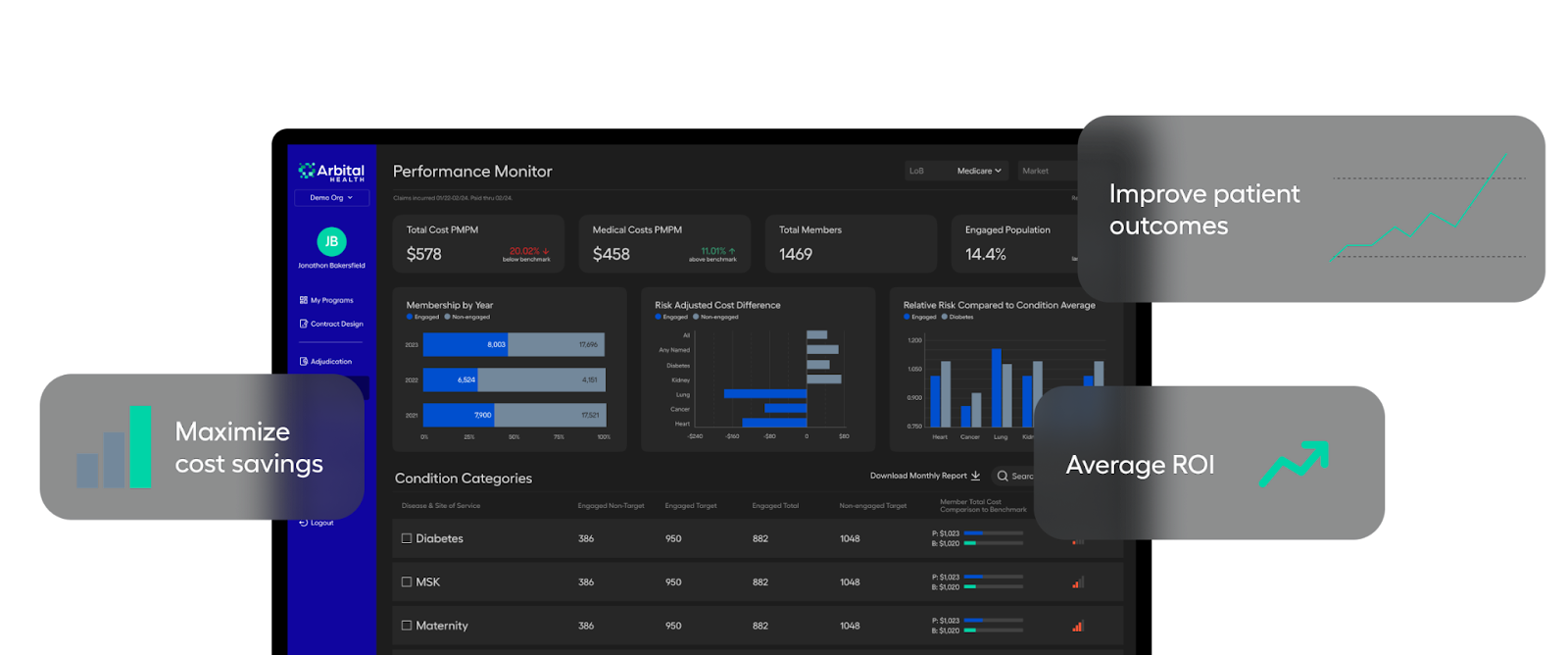
- An overall dashboard of how each program is doing. Total cost, utilization, quality, and pharmacy trend can be sliced by condition, region, site of care, or cohort. The module highlights the share of spend driven by the sickest members, shows whether inpatient or outpatient is pushing variance, and surfaces disease categories where costs are out of line. Benchmarking against digital twins shows whether performance is truly off-trend or simply looks noisy. Here in the graphic above, the benchmark is comparing Disease Condition Categories spotlighting engaged vs. non-engaged patients. Teams can then compare Patient Total Cost (PPPM) to benchmarks, and trigger intensity-based alerts or a signal on the screen to flag hotspots that need attention. Many Arbital customers love the signal on the screen (seen in the very right column as red performance graphs) as a way they can quickly sort to drill down into the VBC programs that need more attention or new disease categories that need to be managed for the patient population.
|
Insights - This is where leaders drill down. If diabetes costs run hot against the benchmark, Insights shows whether it is driven by admissions, ED churn, GLP scripts, or specialty visits. Leaders can dig deeper into understanding engaged versus non-engaged metrics, pivot by facility, by provider group, by plan, by time, or any flag they are tracking in data collected. The module carries longitudinal views, so teams see whether interventions worked and whether variance closed. Additionally, predictive models are included to identify and prioritize members who need interventions. Analysts, actuaries, and clinicians can all self-serve without spinning up a new cube or throwing another ad hoc ticket over the wall.
|
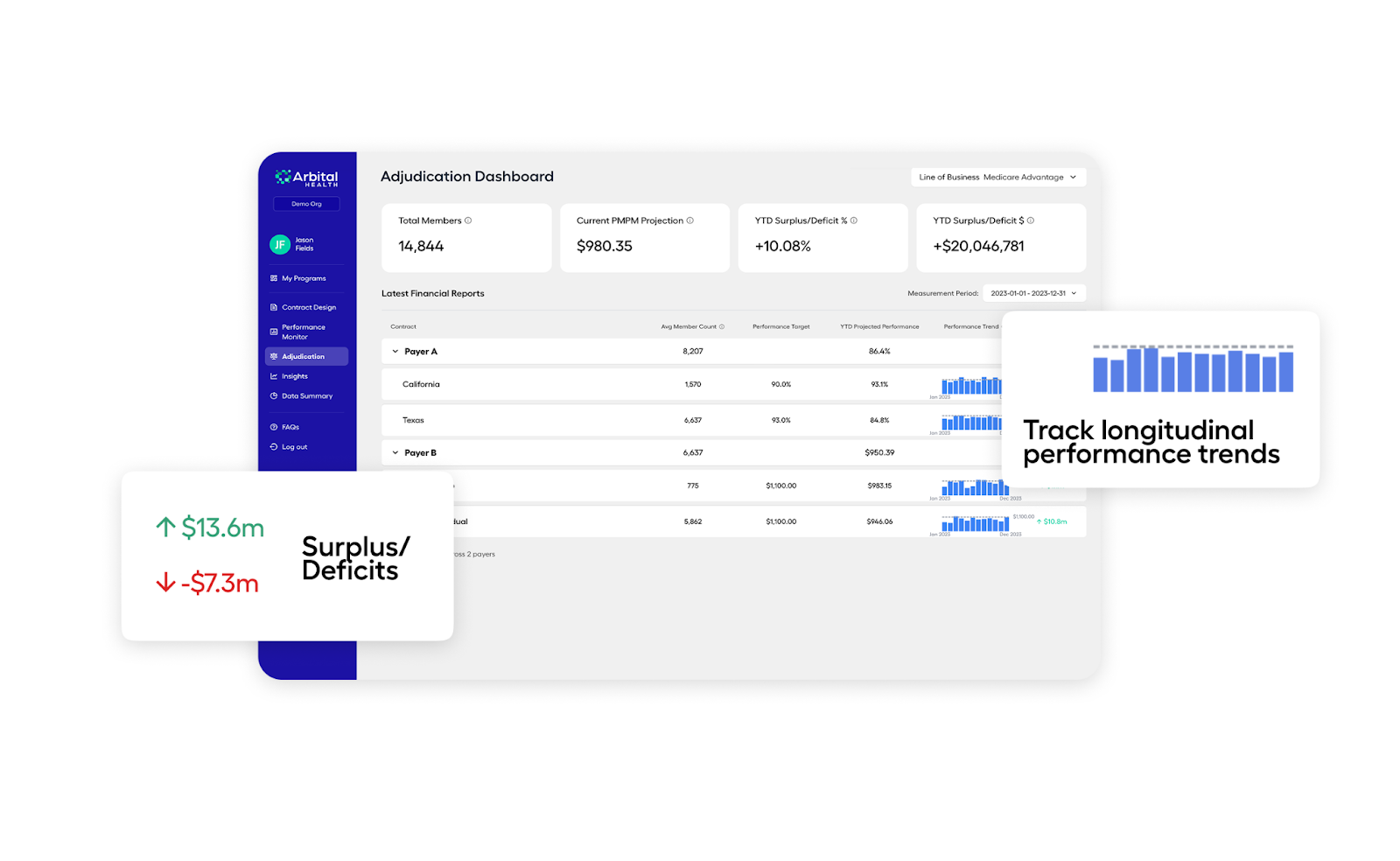
Adjudication and Forecasting - The actuarial heart of the platform. Arbital runs a monthly measurement period for claims completion factors and IBNR off historical lag patterns to project where the contract will end. The system calculates MLR target, YTD Surplus/Deficit %/$, YTD MLR Projection, and applies the exact reconciliation math against the agreement. Finance users adjust assumptions and simulate the effect of specific actions. The tool becomes a flight deck for the last third of the performance year when small moves matter.
|
AI-Assistant, Merlin (in Beta) - And you thought we'd get through this entire feature set and platform overview without talking about AI! In the famous words of Lee Corso, Not so fast my friends. Arbital's AI copilot for its platform, Merlin (which is an incredible AI name, by the way but I digress), sits directly on top of all of your enriched data and codified contract logic. That means you can ask Merlin nuanced questions like PMPM by region, YTD top cost drivers by clinical category, 15-month inpatient admit trends, or flu trends, and it'll return useful information generated into tabular or visually appealing format from your own data, not canned content. The guidance is intelligent, and teams can take this information, validate results, and vastly expedite insights for the rest of the firm. And Merlin is just in the beginning phases of the great unlock in value-based care. No longer will actuary, finance, clinical, and operations teams sit in disparate siloes. These groups will shift from report factories into autonomous decision-makers. In beta today, Merlin is quickly evolving into a fully-fledged support tool for risk-bearing organizations to fluidly assist them with Next Best Actions. In short order, we'll look up and see Merlin helping with more sophisticated tasks (for instance, asking the agent to prioritize a member list for risk of future inpatient or ER admissions and recommending the shortest path to impact and engagement), which will only compound the technological advantage and speed to action for your entire organization. The Arbital told me they're already seeing immediate value-add from Merlin today, even while in beta. They're coming in daily, asking ad-hoc questions in the flow of business, and getting immediate, decision-ready answers from their own data. Canned dashboards still matter, but this conversational GenAI layer takes us to the next level turning static reporting into real-time guidance that improves treatment decisions and truly drives the Triple Aim.
Security and Audit - Every calculation carries an audit trail back to the contract term and the input data. That matters when money moves. Both sides can see the steps. Both sides can explain the settlement.
|
Arbital Health's secret sauce and differentiation |
A few ingredients separate Arbital from typical analytics vendors or bespoke actuarial shops. Critical infrastructure that both sides accept: Arbital is not the plan's tool and not the provider's tool. It sits in the middle with no balance sheet interest in the outcome. That positioning reduces friction when results are close. This lowers the odds that reconciliation turns into a months-long dispute. It also opens the door for multi party arrangements where a plan, a health system, and an enablement firm share incentives and need a referee everyone respects. Actuarial horsepower packaged as product: Arbital blends seasoned healthcare actuaries with software engineers and data scientists. The platform reflects that depth. IBNR methods, completion factors, and settlement logic are not bolted on. They are core. This is not pretty BI pasted on top of loose CSVs. It is contract math that stands up in a boardroom and in a true up meeting. Digital twin benchmarking: As mentioned, a super cool feature set for Arbital customers. The benchmarking dataset lets Arbital match members to peers with similar risk and demographics, then track cost and utilization variance in near real time. That approach produces signals that make sense to clinicians and finance leaders. When oncology costs run above matched peers, leaders can drill into regimens, sites of care, or specific tumor types and take targeted action. That is more actionable than a generic national average. From two contracts to twenty without rework: Arbital turns custom work into a system. Ingest the contract once. Define the measurement libraries once. Add markets and plans without rebuilding the model each time. A health system that used to pick one market a month for deep analysis can finally see the whole portfolio every month. That scale matters when executive teams ask to expand risk posture. CFO and CMO alignment: The platform is the meeting point for financial and clinical strategy. Both leaders use the same tool, the same definitions, the same time stamps. That alignment reduces the classic problem where care teams celebrate improved outcomes while finance reports an unhappy variance. With Arbital, teams see whether a clinical program actually bent the cost curve for the measured cohort inside the active measurement period. Series B as a signal of market pull: Arbital's recent raise fuels deeper payor capabilities and portfolio scale. Plans want a way to standardize reporting to their provider networks, to shorten the feedback loop with providers, and to settle faster with fewer disputes. Providers want a path to add contracts without adding overhead. Enablement firms want a cross payor view that ties clinical action to financial results. The round validates that this shared utility has room to run and capital interest to continue expanding into new features and AI-enabled capabilities. |
Why payors, providers, and risk bearing organizations should work with Arbital |
For ACOs, enablement firms, and other risk-bearing organizations, Arbital aggregates every live agreement in one place and tells leaders exactly where they stand. Take, for instance, one of Arbital's clients who was bogged down by population health and managing risk across a large number of markets. Before Arbital, the chief actuary could analyze one market per month after requesting the data pull from another team. After go-live, the actuary team had a vantage point into not just one, but all markets simultaneously. From there they spotted a pharmacy cost spike in one market, and moved faster to manage the trend. And that's just the financial and administrative side: care teams didn't even need to wait for the actuarial report! They logged in and acted on live data to understand how to care for those patients most appropriately, understand what was driving the cost, and of course, maximize contract value on the back end. For payors and providers, Arbital offers the above and more. Plans face pressure from providers to deliver more actionable, faster reporting. They also want a way to expand VBC with confidence. Arbital gives plans a neutral engine to run downstream arrangements, standardize measurement across networks, and reduce cycle time to settlement. That makes the plan easier to partner with and lowers administrative cost for everyone. For employer plan sponsors, a neutral adjudicator increases trust in outcome based contracts and improves adoption of programs where the employer, the plan, and a vendor share savings. |
The first wave of VBC asked clinicians to do more with less, then handed them delayed spreadsheets and a heaping pile of administrative work. The second wave needs real infrastructure and is aimed at fixing the steaming pile of crap we left with providers on the first go-around. Contracts should read like software configurations. Data should flow into the same model every month. Finance and clinical leaders should work from the same screen. Settlement should feel like closing the books, not litigating a divorce. And value-based care does NOT have to be this hard. Arbital Health is building that operating layer. The company's story is not about shiny care navigation and not about ripping out core payor systems. It is about building the critical infrastructure that takes the gnarly parts of VBC and makes them routine. AI turns a 70 page agreement into structured logic. Measurement libraries classify claims the same way across markets. Digital twins reveal where spend is off trend. IBNR and forecasting turn adjudication into a proactive exercise. Actuaries spend time on strategy. Clinicians get data they trust in time to act. Executives add contracts without adding headcount. Keep an eye on Arbital as they scale from their Series B and beyond (and I'm fairly certain they WILL scale beyond). They're operating in an area of sore need. Value-based care will always involve messy human work, complex patients, and tradeoffs between sites of care. But the paperwork and math do not have to be messy, too. Arbital's bet is straightforward. Build a shared utility for adjudication and performance, get everyone on the same truth, and the shift to value accelerates. The market is voting that this is the way forward. For operators weighing next steps, the takeaway is practical. If you plan to grow risk posture over the next two years, put infrastructure in place that scales. If your finance and clinical teams work from different numbers, fix that. If your organization waits months to know whether you are on target, shorten the loop. Arbital Health exists to make those moves possible, not with a shiny front door, but with the rails underneath that carry the weight. Get in touch with the Arbital Health team today |
|
|
Thanks for the read! Let me know what you thought by replying back to this email. — Blake |
|
|
.png) | Share Hospitalogy, Earn Rewards | Have friends who'd love Hospitalogy too? Click the link below to share Hospitalogy with your friends and earn awesome rewards! | |
|
PS: You have referred 0 people so far | | Share Hospitalogy! | |
|
|
|
|
Get your brand in front of 48,000+ executives and healthcare decision-makers. |
I'm building a community of leaders in strategy, finance, and ops
at hospitals and health systems to help us connect, learn, and grow together. |
Workweek Media Inc.
1023 Springdale Road, STE 9E
Austin, TX 78721 Want to ruin my day? Unsubscribe. |
|
|
|







No comments