Happy Thursday Hospitalogists!
Today's is a quick one on Ballad Health's recently released operating and financial overview for their fiscal year ended June 30, 2025. After reading I thought it would be worthwhile to jump into since many of the issues affecting Ballad Health (including Ballad's management commentary section on the 'behavior of insurers' with downcoding and denials) are being felt by many providers across the country.
Let's jump in. |
Was this email forwarded to you? |
|
|
Going deeper on an interesting topic, theme, or trend |
As many of you probably know, Ballad Health, which formed in 2018 under a COPA arrangement, has been in the news in the past for its unique positioning as a Tennessee sanctioned monopoly in rural parts of Kentucky, Tennessee, North Carolina, and Virginia. |
When weighing something like a COPA for Ballad Health in rural America, state officials and policymakers have to weigh the decision based on the following: - Do we want these communities to have any local access to healthcare and keep these facilities open despite worse quality and a lack of competition?
- How can we introduce checks and balances to a healthcare regional monopoly?
As it turns out, Tennessee and Virginia approved Ballad's COPA because policymakers determined that, under certain conditions, the benefits to keeping the facilities opened outweighed potential ramifications of anticompetitive practices, consolidation, and any possible deterioration in quality. Over the years Ballad Health has received scrutiny for this special structure especially related to its quality metrics, and the Tennessee Department of Health has gone through several iterations of negotiations with the health system, implementing a scorecard-based approach where quality has increased in weighting. Ballad also has to disclose a ton of information to the state on an annual basis, which makes the health system interesting to study overall. The problem with that is one you might expect…it's hard to measure quality. How do you define quality? The two parties have gone back and forth on what quality metrics should be included, and how heavily weighted those quality metrics ought to be. This year, based on that linked article above, the scorecard weights quality of care at 40%, though the measures are now pass-fail rather than scored from 0 to 100. It's like I'm taking a college class all over again, except we're talking about actual patient outcomes and not my shitty Greek Mythology grade (don't ask). Anyway, to simplify things a bit, all you need to know is that Ballad Health holds a unique position in the health system world as a monopoly, this dynamic in and of itself is controversial, and has yet another stakeholder to negotiate with on an annual basis besides payors - COPA policymakers. And the goalposts constantly shift - in either direction. Because of all of this ongoing hubbub, Ballad has received a ton of negative press from the likes of KFF. And this press again begs the question - do you want these facilities accessible and open; because otherwise the healthcare facilities would be unsustainable on an unconsolidated, standalone basis given the high fixed costs, volumes, and labor needed to create a sustainable operation. Honestly, I would love for Hospitalogists' thoughts on alternatives to this model, or what better policy might look like, and what rural healthcare providers have to work with at all given the shredded band-aid they just received from the OBBA, because I have none of those answers. |
Under the Hood of Ballad Health and Level of Care Adjustments |
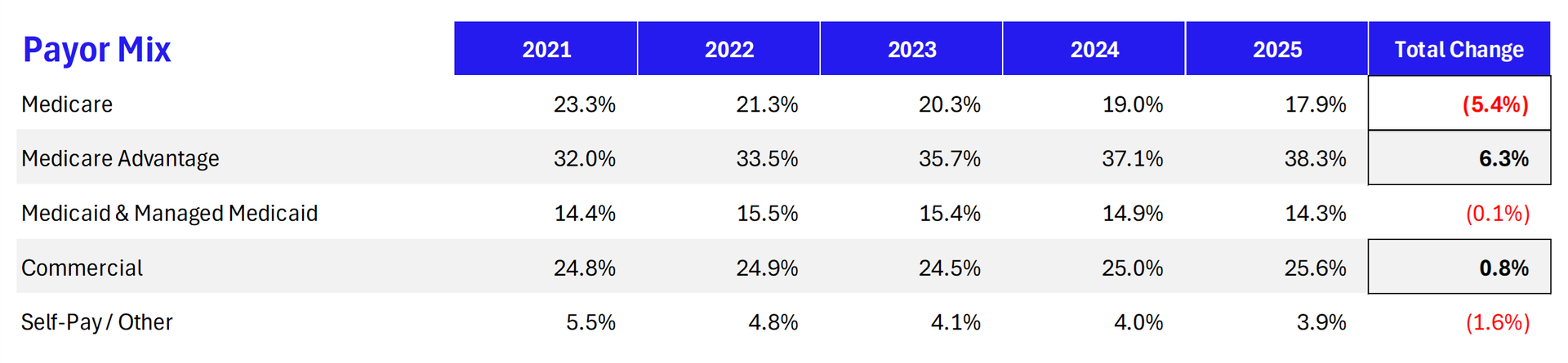
Moving on from this commentary, for this newsletter I'm going under the hood of a monopoly to focus on Ballad's most recent fiscal year end and the management commentary therein. Because when a provider is perceived to have certain advantages, payors take notice. Taking a look first at Ballad's payor mix (which is unmarked but I'm assuming to be based on net revenue) - Ballad is seeing a big jump in Medicare Advantage patients: |
Ask any healthcare executive and they'll tell you MA pays you 95% or lower on the dollar versus traditional Medicare for patient care. The reduction in payment is indirect through denials, added administrative costs…and now, behavioral down-coding or 'level of care' adjustments, as Ballad Health puts it. We're seeing a convergence of a couple trends here, and maybe even more beyond this: - AI upcoding bots are optimizing coding and documentation, leading to higher reported acuity and therefore higher dollar claims.
- Medicare Advantage continues its penetration and growth versus traditional Medicare, and despite recent headwinds, political rhetoric supports MA overall. The trend will negatively impact hospital and health system payor mixes like we're seeing with Ballad Health
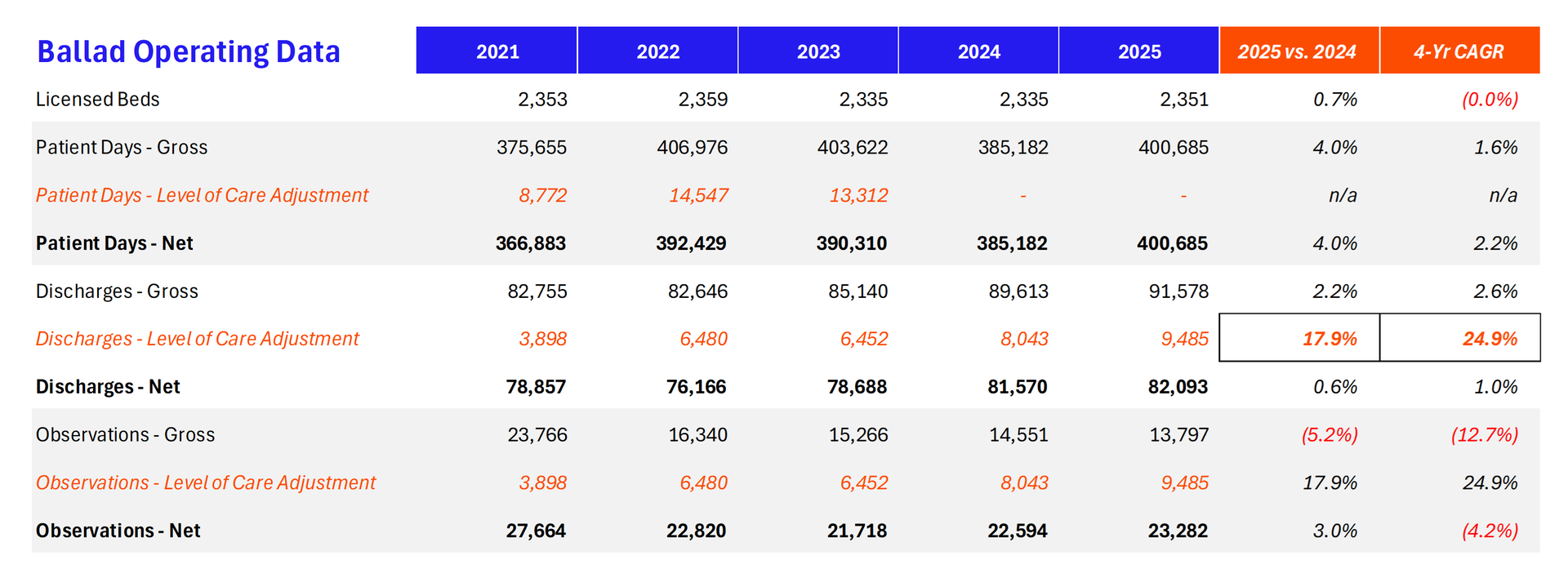
As a result, payors are coming out with aggressive new reimbursement policy to oppose upcoding, implement utilization management tactics, and try to get their medical costs under control to turn a profit in MA lives. Some recent attempts we've seen included Cigna's new auto-down-coding policy and Aetna's 'low-severity inpatient' cut to low acuity inpatient reimbursement, where Aetna plans to retroactively deny inpatient admissions, deeming them unnecessary and reclassifying these 'unnecessary' admissions as outpatient observation stays - a classification hospitals lose money on. Back to Ballad Health. The bulk of Ballad's management commentary was spent on this specific issue. Ballad Health is experiencing Medicare and Medicaid payor level of care downgrades, from inpatient admissions into observation stays, a problem only exacerbated by increasing MA patients: |
- As reported nationally, there is a growing trend by certain insurance companies serving populations in the Medicare and Medicaid program that have increased their systemic denials of claims and unilateral "downcoding" or retroactive level of care downgrading after the patient has been discharged from inpatient care…Annual level of care downgrades have more than doubled from 3,898 in FY2021 to 9,485 in FY 2025. These level of care downgrades often lead to increased patient out of pocket cost for Medicare Advantage consumers as well as a significant reduction in net revenue for the hospital.
- Ballad noted a 79% increase in level of care downgrades when comparing Q4 2025 to Q4 2024. You can see the trend in the table above as reported by Ballad - payors reclassified 10% of their discharges to observation status.
- The increase in level of care downgrades and denials from Medicare Advantage insurers results in an aggregate reduction in revenue of up to 15 percent when compared to traditional Medicare.
Ballad also goes on to say that the increase in denials and approvals from payors has also affected its length of stay for MA patients, causing these patients to be in the hospital longer and resulting in unprofitable observation days along with increased ER pressure while they wait on new care setting approval. So who's right? It's impossible to know. We should trust that the ER physicians and clinicians and protocols are making the right choice in admitting patients to the hospital, but payors also do serve as a check and balance on aggressive admissions policies. Plus as a rural health system and monopoly Ballad has a vested interest in getting as much downstream volume in the door as possible since there is literally no other care choice. It's tricky when you get into the details, isn't it? And I'm not even in either of their shoes actually trying to navigate all of this. The problem is that we're solving for financial viability with these decisions and not necessarily what is best for the patient. How might these dynamics play out over time? - Maybe we'll see some sort of neutral authority AI 'Switzerland' sit in the middle of denials, prior authorizations etc. The best AI bot shouldn't win - the best care should win.
- As this continues we'll see programs like hospital at home or other care coordination measures to push borderline inpatient and observation cases out of the hospital into the home or into excess capacity.
- Provider organizations will rally their communities and physician / clinician bases to oppose these policies as we've seen time and time before.
Ballad Health is a state-sanctioned monopoly, so while they have their own challenges with poor population growth and the above, the rest of you will have to contend with these dynamics in much different and more competitive environments. Because unfortunately down-coding practices negatively affect the provider organizations who aren't gaming the system. And there's nothing you can do about the secular growth in Medicare Advantage. Still, at the end of the day, all of this administrative nonsense detracts even further from providing value to patients and aligning financial incentives with patient outcomes. We should all be striving toward a future where the patient is at the center of these conversations. Business often gets in the way. |
|
|
SPONSORED BY INNOVACCER 80% of AI pilots fail to produce returns. Why? Because people, process, governance, and data aren't ready. My latest deep dive shares a smarter way forward with: Get a closer look at how Innovaccer Gravity helps you implement AI with real ROI. |
|
|
Texas has a bye this week, and it's my son's second birthday, so I'm coasting into the weekend. Good luck to your respective teams this week, and wish me luck on smoking 13+ pounds of pork shoulder! Any tips appreciated. I know you're out there. |
|
|
Thanks for the read! Let me know what you thought by replying back to this email. — Blake |
|
|
.png) | Share Hospitalogy, Earn Rewards | Have friends who'd love Hospitalogy too? Click the link below to share Hospitalogy with your friends and earn awesome rewards! | |
|
PS: You have referred 0 people so far | | Share Hospitalogy! | |
|
|
|
|
Get your brand in front of 49,000+ executives and healthcare decision-makers. |
I'm building a community of leaders in strategy, finance, and ops
at hospitals and health systems to help us connect, learn, and grow together. |
Workweek Media Inc.
1023 Springdale Road, STE 9E
Austin, TX 78721 Want to ruin my day? Unsubscribe. |
|
|
|






No comments