PARTNERED WITH  |
|
|
Happy Tuesday, Hospitalogists! I'm excited to be at HLTH this week. Let me know if you're around, I'd love to say hi. And, for the rest of you who I can't chat with in person… we have Ask Hospitalogy. A new newsletter segment where I'll share perspectives from fellow healthcare leaders on anonymous questions you submit about pressing challenges, opportunities, and trends you're seeing in the space. My ask: Drop an anonymous healthcare question or musing here for a chance to have it featured in the NL and discussed by your fellow Hospitalogists! Speaking of challenges, today we're talking about tackling the big hairy problem of prior auth. Let's get into it. |
Was this email forwarded to you? |
|
|
The most important news from the week |
Cracking the Prior Auth Code: Trust, Tech, and the End of Red Tape |
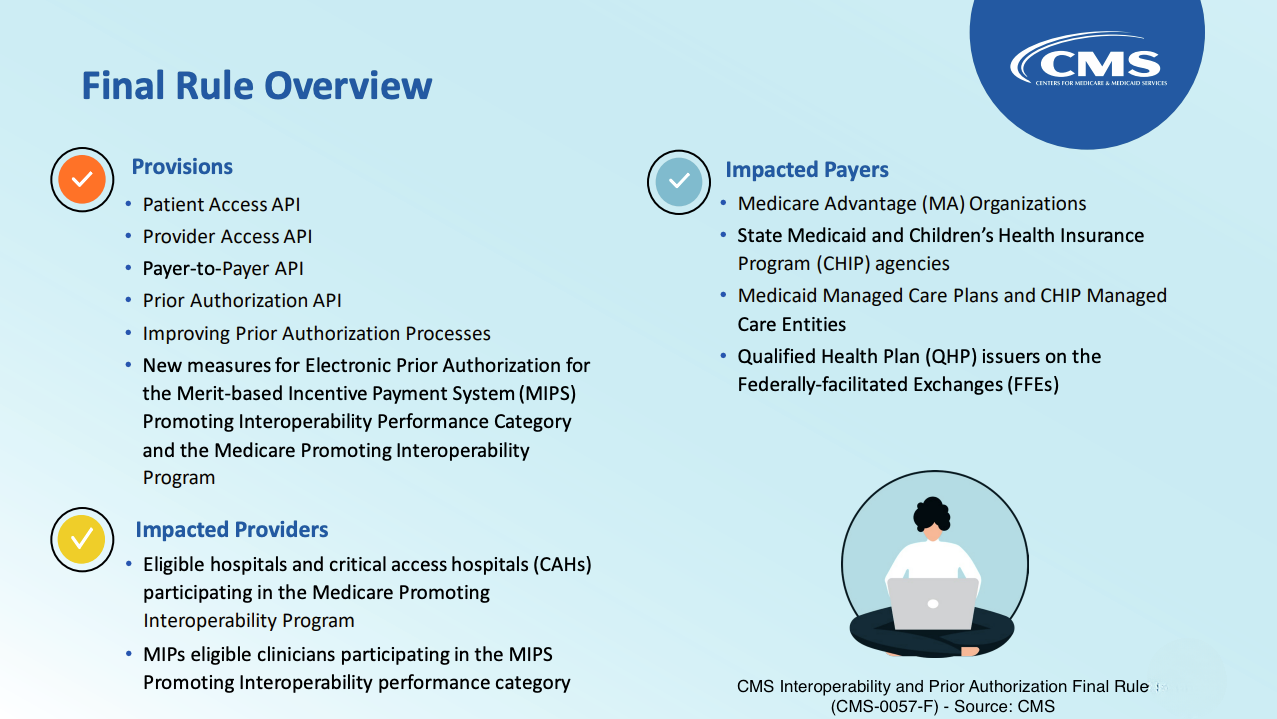
If you lead a hospital or health system, you do not need a 101 on prior auth. You need a map for the next 18 months, because the ground is shifting. The public is angry, regulators are moving, and Medicare fee for service is testing utilization management with AI in six states as soon as 2026. That means the administrative fight you associate with Medicare Advantage is about to creep into your traditional book of business. The narrative isn't confined to the trade press. One story still ricochets around board rooms. Austin plastic surgeon Elisabeth Potter says she stepped out mid-reconstruction surgery after UnitedHealthcare rang the operating room asking her to justify an overnight stay. UnitedHealthcare says it would not expect a physician to interrupt care and later pointed to a hospital error. Either way, the clip went viral and the incident became a symbol for a broken process. For leaders, that is the brand and political context your organization is operating in. Add in new CMS interoperability and prior authorization rules that set clock speed and transparency expectations starting January 1, 2026, with additional API requirements through 2027, and you have reputational and regulatory pressure to modernize. |
Where We Are: A Messy Market with Real Money at Stake |
There is no single prior auth market. There are overlapping regimes across Medicare Advantage, Medicaid managed care, exchange plans, commercial lines, and soon slices of Traditional Medicare. Each line comes with its own rules, portals, and clocks, creating an administrative overload that is compounded by rising utilization trends among seniors. A 2024 AMA survey found physicians and staff spend about 13 hours a week on prior auth, handling roughly 39 requests per physician. |
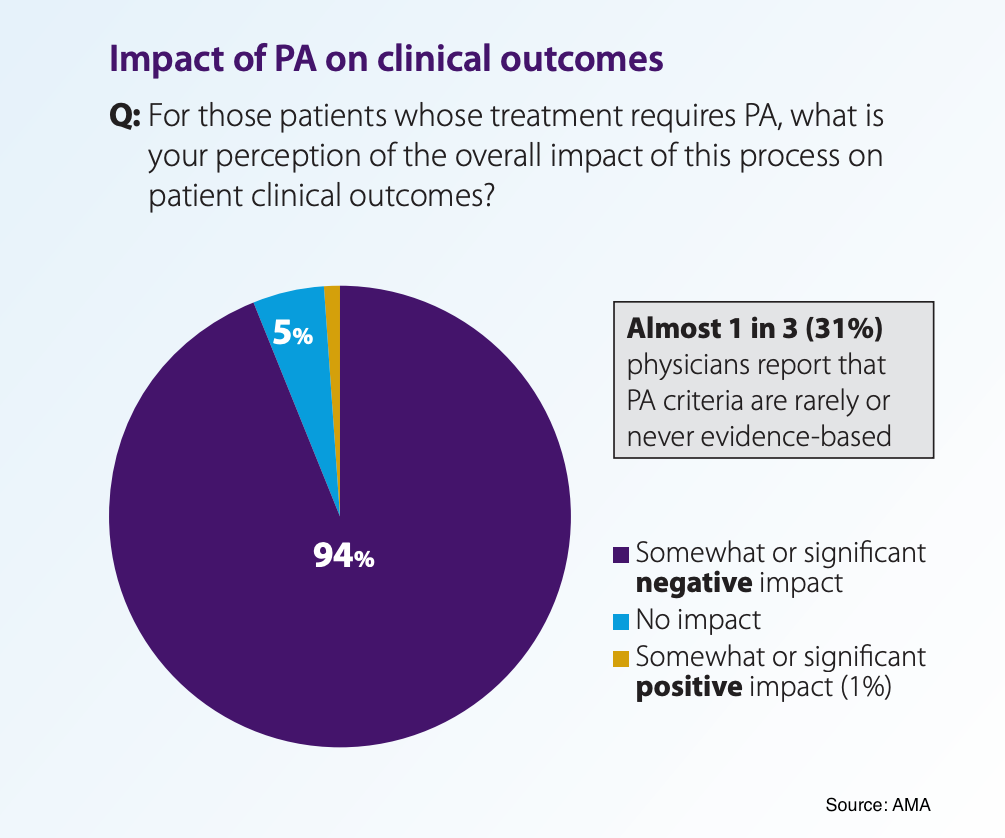
In marketplace plans, payors denied 19% of in-network claims in 2023, and physicians report widespread delays in care. Those are not anecdotes. They are measurable headwinds to throughput, revenue, and patient experience. Laden with a ton of bad press and worse operating decisions, insurers are moving to reset the optics. Humana says it will remove about one third of prior auth requirements for outpatient services by 2026. Aetna created a program that reduces PA requirements for over 1,000 providers based on consistent UM performance. Automation is being introduced to streamline approvals for prescriptions and procedures with historically high approval rates. I know what you're thinking. Insurers are incentivized to implement UM, especially in the current environment. But nevertheless, it's still interesting and notable to understand where the puck is moving and see, at the very least, what they say they're doing. And what they're doing is moving UM programs from blanket denials and gatekeeping into smarter, rules-based triage approaches. |
Why This Matters to Leaders Now: the P&L Is In the Workflow |
Labor still dominates the hospital cost structure. Total compensation and related expenses account for roughly 56% of hospital costs. Every extra hour your teams spend in fax land shows up in either overtime, contract labor, or lost clinical capacity. Do a quick sensitivity check: - If administrative staff time truly averages 13 hours a week per physician and you employ 100 physicians, that is 1,300 hours a week. At a fully loaded $32 an hour, you are spending about $41,600 weekly, or just over $2.16M annually, on forms and follow ups. That figure ignores physician time and downstream leakage from delays.
- Denial math bites twice. Even if a portion of denials are ultimately overturned, most offices do not appeal every case, and the cycle time chokes cash. There's also a huge variance in denial rates by payor. That volatility becomes your working capital problem.
- The program risk is expanding. Traditional Medicare's pilot means UM logic will cross lines of business. Waiting to react is not the answer. Your clinical, IT, and revenue cycle teams will need one playbook that works for MA, commercial, Medicaid, and parts of fee for service Medicare.
|
Where It Hurts: Five Knots That Choke Throughput and Margin |
1. Fragmented rules and channels
Your teams bounce among portals, PDFs, phone trees, and faxes. Integration into the EHR is the exception rather than the rule. That kills first pass yield and extends DSO, while consuming the most expensive line on your income statement. 2. Opaque criteria and slow clocks
Health plans may use proprietary or outdated clinical guidelines. Decisions may arrive without clear clinical rationale, leaving providers and patients in the dark. It's a vicious cycle that can lead to more denials, avoidable appeals, and case deferrals that spill into avoidable admissions. Expect more plans to publish turnaround and approval metrics as CMS transparency requirements kick in. |
3. Prior auth as a clinical bottleneck
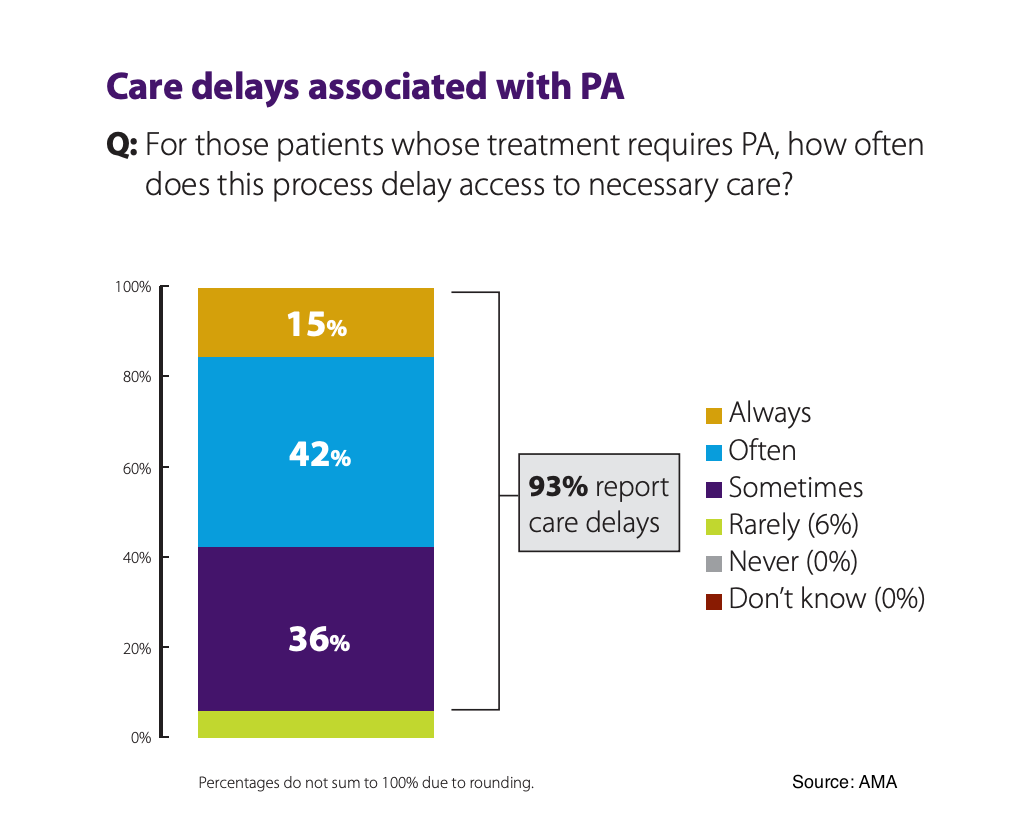
93% of physicians report prior auth delays care. Along with potential for patient harm, care delays add length to clinical pathways, which increases no shows, OR idle time, bed day variability, and readmissions risk. |
4. The manual burden tax
Every unit of manual rework shows up as extra FTEs or vendor spend. Look at your last 12 months of denial write offs tied to authorization and medical necessity. The silent line item is the opportunity cost of missed cases when clinicians reduce volume to offset administrative drag. 5. Cross-market inconsistency
You cannot scale staff expertise if each plan and line of business demands a different rule set. Training costs rise. Error rates rise. Adoption of tools lags because workflows differ by payor. That shows up as variance in service line margin by payor mix. |
What's Working: Trust… With Checks |
Trust contracts, not prior auths
One interesting shift is the move to trust-based models for high-performing groups. UnitedHealthcare's National Gold Card waives clinical documentation review on specific services for groups that consistently meet evidence adherence thresholds. Some payors use tiered trust models to make the process easier for high-performing providers while those with outlier patterns remain subject to standard protocols. Retrospective audits
Oversight doesn't disappear; it just shifts from pre-approval to retrospective audits on a sample of cases. MCG, InterQual, and specialty managers like HealthHelp codify rules and can drive retrospective audit or prospective guidance. These are the building blocks inside many payor and provider platforms. Automate the obvious
Where the historical approval rate is sky high, automation makes sense. Surescripts and Optum Rx piloted touchless prior auth that dropped median turnaround from 8.5 hours to under 30 seconds and slashed appeals and information-related denials. GuideWell reports 78% of authorizations approved within 90 seconds after plugging AI into the process. These are payor-side examples, but they reflect the standard providers will expect in the EHR. Put the rules in the chart
Cohere Health's integration with Epic's Payer Platform lets clinicians initiate authorizations from the ordering workflow and apply payor policy in real time. Innovaccer is pushing agent-style tools that pull payor requirements, assemble packets, and submit from inside the record. If the criteria are embedded at order entry, you reduce the need for a separate prior auth function and increase first-pass approvals. Targeted simplification that clinicians actually feel
Aetna says more than 95% of eligible PAs are reviewed within 24 hours and is bundling multiple MRI or CT authorizations into a single up front approval for certain cancer patients, with plans to extend bundles to cardiology and MSK. Humana plans to cut about one third of outpatient PAs by 2026. These examples change cycle time and reduce touches. A rethink of reauthorizations
Last year, Optum Rx launched an initiative to eliminate up to 25% of reauthorizations to simplify how patients with chronic conditions receive their medications. It started with approximately 80 drugs for various chronic conditions, followed by 60+ additional drugs in July 2025. Clinical decision support as UM by another name
Geisinger used EHR alerts to reduce expensive lab orders with a measurable drop in high-cost tests. When done well, CDS aligns provider ordering with payor policy upstream and lowers the prior auth hit rate without a fight. A constantly evolving healthcare AI landscape
Elion keeps a living market map of prior authorization and utilization review vendors across payor and provider workflows. Scan it if you want a sense of how fast the space is moving and how many "better bots" are chasing the same prize. |
Open Questions Leaders Should Push On |
Prior auth isn't going anywhere, but it is evolving. We're moving from a blunt, bureaucratic hammer to something more like a programmable guardrail. The winners will be the systems that can actually prove they're responsible stewards of limited capacity, with clean data pipelines and automated workflows built into the EHR. Everyone else? They'll keep adding FTEs, burning hours on hold, and wondering why their operating margins keep circling the drain. 6 questions to push on: - What share of my prior auth volume can I move to instant or near instant decisions in the next 12 months, and what is the dollar impact on labor and throughput?
- Which payors will sign trust-based agreements tied to retrospective audit and what data do they need to say yes?
- Where can clinical decision support quietly reduce the need for prior auth in the first place without provoking a clinical revolt?
- How will my operating model change if Medicare fee for service expands prior auth beyond the initial pilots?
- What single source of truth will my system use for payor rules, with governance to keep it current and clinically credible?
- Am I prepared to publish my own internal metrics on authorization cycle time and patient impact so I can hold vendors and plans to the same bar?
|
|
|
Thanks for the read! Let me know what you thought by replying back to this email. — Blake |
|
|
.png) | Share Hospitalogy, Earn Rewards | Have friends who'd love Hospitalogy too? Click the link below to share Hospitalogy with your friends and earn awesome rewards! | |
|
PS: You have referred 0 people so far | | Share Hospitalogy! | |
|
|
|
|
Get your brand in front of 49,000+ executives and healthcare decision-makers. |
I'm building a community of leaders in strategy, finance, and ops at hospitals and health systems to help us connect, learn, and grow together. |
Workweek Media Inc.
1023 Springdale Road, STE 9E
Austin, TX 78721 Want to ruin my day? Unsubscribe. |
|
|
|







No comments