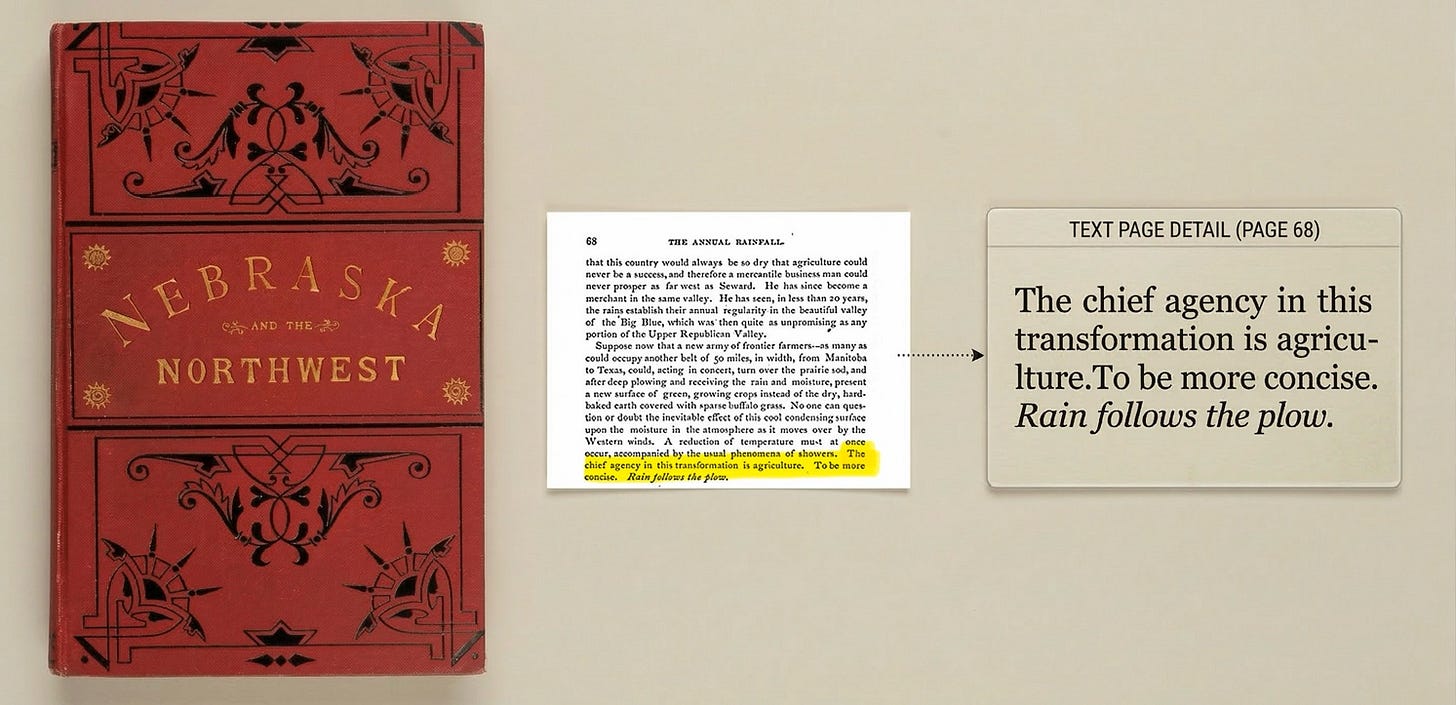
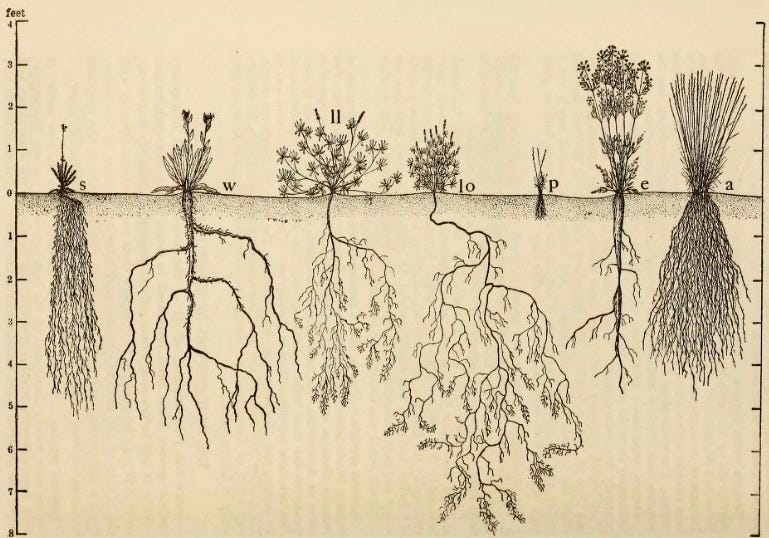
The wheat was fine. The root structure that made the land fertile had been stripped out in pursuit of faster yield, and no amount of capital or conviction that rain follows the plow could substitute for what was gone. The farmers who survived the 1930s were the ones who had studied what the land could actually support, who understood that what a piece of ground can grow is determined below the surface.
Every complex system has root structure that outsiders cannot see, and insiders take for granted.
All that's really new in 2026 health care is the conviction that large language models and AI agents have collapsed the timeline. When I walked the exhibit hall at ViVE and HIMSS this year, the pitch was the same at every booth. AI has become the new vehicle for old hopes. For the better part of two decades, digital health has promised the orchestration layer that finally makes the system behave like a system. The ambition is not new. The certainty that this time the technology will deliver it is the strongest it has ever been.
U.S. health care does not move slowly because the people inside it are slow, though a deep strain of risk aversion trained into it contributes more than many appreciate. It moves slowly mostly because fee-for-service reimbursement pays for volume rather than outcomes. No single fact shapes the system more than this one. The entire institution is organized around a business model that rewards doing more, and it has been organized this way for decades. Until that structure changes, most of what gets built on top of it is decorative. Many misread the friction as a slow sales cycle. It runs deeper than that. How the United States pays for care determines what any technology can actually do once it's inside.
I recently watched a company demo an AI care coordination platform. Impressive product, well-funded company. Someone asked what happens in settings where primary care physicians are on a productivity model that gives them fifteen minutes per visit, and the platform's recommended actions require time that doesn't exist in that model. The founder gave an answer about workflow integration. It didn't change the fifteen minutes.
Some of what AI does in health care works right now, and it works for a specific reason. LLMs are language machines. Physicians are drowning in language: notes, messages, prior authorizations: the documentation load that multiplies every year. The relief is immediate and usually measurable in the same way it's measurable for anyone whose daily work involves processing large volumes of text.
Revenue cycle management, structured and high-volume, is the same. They pay off inside existing workflows because nothing underneath needs to change.
The orchestration play is something else. The company that promises to become the intelligent layer across the care continuum, coordinating payers, providers, and patients through a set of AI agents. That requires everything underneath to change: workflows and the fundamental economics of how health care works. The technology may be ready. But the system absorbs change at its own pace, and no improvement to the technology accelerates that, especially when the underlying business model is the same.
This is not true everywhere. Sequoia's early bet on Stripe reshaped payment infrastructure on a fund's timeline. A developer choosing Stripe over a legacy processor loses nothing and gains everything on day one. Rain followed the plow. A health system adopting an AI platform still gets paid the same way it did yesterday. Health care's customer cannot adopt differently until it is paid differently, and no amount of deployed capital changes that from the outside.
VC fund economics compound this. The degree varies by stage and mandate. But the pattern is consistent: a fund with a deployment clock needs companies that show traction on a timeline that brings value like the next markup. Health care resists the timelines capital needs it to follow, and bigger funds intensify the pressure because the acreage they need to plant across expands with every raise.
So the narrative stretches to fill the gap. The pitch becomes about the world as it should be rather than the world as it is. Meanwhile the deployment schedule assumes the system has already transformed. There are suitcase farmers in health care. Funds with GPs that have never walked the halls of a health system, backing companies with no institutional knowledge or contracts, planting from a distance, returning only to collect.
In venture, conviction is the highest compliment. It applies to investors and founders alike, the fund that bets before consensus and the founder who builds or pivots through the trough instead of caving at the first headwind. In health care, conviction without root knowledge breaks ground fast. What blows away is everything that was holding the surface together.
The system's desire to do better is almost always genuine. I work with people who chose this field because they wanted to take care of patients and with builders and investors who spend their days up against economics that make it harder than it should be.
The founders who will build durable companies in health care have spent enough time inside the system, or selling to it, that they've stopped believing rain follows the plow. They know what can grow depends on what's underneath, and that changing what's underneath is generational work. The companies that last will be the ones that found ground that can already support what they plant.
The conviction that we can invent our way out of problems that we have spent a century building is an especially American strain of optimism.
The southern plains produce more wheat today than they did in 1929, but on thinner soil, supplemented by aquifer irrigation and synthetic fertilizers. The root structure never fully came back. What did come back took decades of contour plowing, shelter belts, and cover crops. Unglamorous things. No one called them innovation at the time.
Jonathan R. Slotkin, MD
Co-Founder and General Partner, Scrub Capital
Chief Medical Officer for Strategy and Growth, Geisinger
Practicing Neurosurgeon











No comments