PARTNERED WITH 
|
|
|
|
Hospitalogists, another Thursday is upon us, and earnings season is here. We’ll dive into that next week, but for now, I have a great guest essay from some smart, thoughtful folks in healthcare - Chrissy Farr and Mike Desjadon. They took a crack at one of the biggest looming friction points in healthcare around AI, innovation, and job displacement, which is something I’ve touched on in the past. Would love your thoughts as they propose some solutions to this problem!
Let’s dive in.
|
Was this email forwarded to you?
|
|
|
|
SPONSORED BY AMPLIFYMD
Health systems often rely on high-cost locums and other temporary staffing models to manage specialist shortages, but that doesn’t solve the underlying coverage problem.
AmplifyMD's white paper shares real-world examples of how hospitals are using tech-enabled virtual care models to improve specialist access, reduce dependence on temporary labor, and better utilize scarce physician resources across multiple facilities and service lines.
The paper explores:
The growing cost of long-term locum dependence Why one-physician-per-site staffing models are increasingly unsustainable How virtual specialists support lower-volume hospitals and hard-to-fill specialties The benefits of scalable workforce optimization, including the financial impact of reduced transfers, lower patient leakage, improved throughput, and better specialist utilization
See how provider coverage tailored to meet actual demand enables hospitals to stop being reactive and start building long-term clinical capacity.
|
|
|
|
Addressing the Economic Reality of AI Transformation in Healthcare |
The narrative about the AI-driven transformation of healthcare has grown increasingly utopian. Patients will be empowered through faster diagnoses. Doctors will be freed from administrative hassle and paperwork. More efficient systems will deliver higher margins.
What's missing from the conversation is the inevitable fall out: the billing clerk in rural Kentucky who has held their job for eleven years, is now no longer needed. The hospital around which that town’s economy revolves will soon be in a position to cut staff through layoffs. The medical coder in a small Ohio town will falter on their mortgage payments after being replaced by AI. A recently laid off registrar at Mount Sinai can no longer support their family, because they live in one of the highest rent cities in the country.
We are not talking about them right now because we think healthcare will be one of the last holdouts when it comes to massive job-related dislocations. Many healthcare workers are supported by strong labor unions and employed by not-for-profit health systems that have insulation from economic trends. The life-and-death stakes of the industry means it will likely proceed cautiously when it comes to AI.
Those insights all have an air of truth. But it's also true that administrative costs in healthcare are now more than $1T annually. The federal safety net is buckling under its weight and at least half this cost is automatable. Cuts are coming. They may not be as swift as what we are seeing in other industries, but eventually executives will make this shift. Much like Ernest Hemingway went broke, it will happen gradually, then suddenly.
So let's be honest about what's coming. Predicting the future through rose-colored glasses only serves the glasses manufacturer. AI will displace many jobs in healthcare. Those job losses will impact communities. Executive stakeholders will protect their workers until their bonuses are tied to reductions in force. Unions will protect the 13% of healthcare workers who hold cards, but everyone else will be vulnerable. There’s no protection for the rural hospital that quietly contracts out its administrative functions to a software vendor or the urban hospital facing tanking margins due to uncompensated care and Medicaid cuts.
Jobs most vulnerable to displacement are the ones behind the scenes: medical coding, prior authorization teams, transcription, scheduling, billing and administrative intake. Many of these functions are automatable because they involve task-based, repetitive manual work. Some are already being automated, or the role has been outsourced. Sure, some of these roles will evolve to being more focused on performance and specialized areas, like exception management - but the pull is net reduction. Automation will be deflationary, which is not a bad thing. But job loss is. And focusing on cost reduction doesn’t absolve us from having a community-focused plan for when this happens.
|
Here’s what makes this a moral issue and not just an economic one.
When a coding nurse is employed in a community, their salary circulates there. The nurse buys groceries, pays rent, and money goes into the local tax base. When that coding nurse is replaced by AI, her economic activity disappears into a server farm. The efficiency gain is real, communities that are already struggling lose. We tend to count the first one and ignore the second. AI will create as many or more jobs than it replaces, just like every other technology. But those new jobs might not come to these towns or to laid-off workers. Job dislocation will happen at a faster speed than re-employment - and even when re-employment occurs, it is unlikely to be tied to the physical footprint of a health system.
Unlike the de-industrialization of the 80s and 90s,these job losses won’t just happen in a handful of places forgotten by those who caused it. They will happen in every town and every city, blue and red alike. The Roanoke Valley in Southwest Virginia can no more absorb half of Carilion Clinic’s 13,000 employees losing their jobs than New York City can absorb half of the 400,000 people employed across its five largest health systems. Job losses at this scale won’t be merely sad, they’ll be destabilizing at a scale we haven’t yet begun to reckon with.
First, we must name the problem: People are losing jobs, and that will have a detrimental impact on communities. But we still have the time to work towards solutions that are humane,empathetic, and realistic. The alternative is to ignore the problem because it feels too distant, or too political.
|
What does transition look like? |
We’re proposing a healthcare workforce transition plan. We’d like for our industry— across the worlds of policy, technology, AI and healthcare— to come together to discuss what that looks like in more detail. As of 2026, there's no equivalent of the trade adjustment assistance programs — however inadequate — that at least acknowledged factory workers deserved something when their jobs moved overseas.
Our first few ideas are below,, and we’d love to hear yours.
|
1. Ensure that efficiencies gained will flow to real people: |
Automation could realistically save the US economy trillions of dollars in waste, fraud and inefficiency in healthcare. These dollars have to translate to lower “price at the pump” in healthcare and not just better margins for private-equity backed companies. These folks can’t lose their jobs and also get slammed with ever more expensive healthcare.
|
Related to the above, the rapid adoption of these technologies will create efficiencies with positive financial impacts. Those must be captured and reflected in lower financial outlays per capita. Over a period of time, a portion of that can be distributed to these workers who paid for the future with their roles, in the form of severance.
|
3. Codify job preference for workers in health fields |
We already do this, as we should, for women and minority owned businesses. We can do something similar for these workers in a manner not-dilutative to that effort.
|
4. 21st Century Works Act |
Just as the Cures Act authorized $6.3B in federal funding over 10 years to advance biomedical research. We should do the same to create the healthcare workforce of the future, and prepare new and existing workers for it. One of the ideas that came up at a recent HFMA conference we attended for heads of revenue cycle and hospital CFOs? Health systems may have hundreds of people focusing on tasks that can be automated. But there remains a shortage of people who can care for patients at home, or drive vulnerable seniors to medical appointments. There may need to be a reallocation from purely administrative roles to those focused more directly on patient care - and this would be a good thing!
|
Trade schools are already seeing a boon because of AI, but with a focus on the role these schools can play in skilled trades. These institutions can play a critical role in training the healthcare workforce we will need moving forward: roles that are sustainable and which will be desperately needed. We won’t need quite so many radiologists or pathologists. But there will be an enormous need for geriatricians as our population continues to age, or social workers and nurses that are involved in hands-on patient care - and even paid caregivers who may not need advanced clinical degrees.
|
6. Positioning innovation SWAT teams at the frontlines of care settings |
Historically, hospitals were competing with (and often losing to) technology companies for technical talent. Now, because of AI, hospitals can equip the teams they do have to handle much of this work, increasingly cut ties with vendors, and bring more of their efforts in house or centralize relationships with a comprehensive partner. Health systems should nominate small teams of people to get very comfortable with using AI tools, giving them time and resources to move quickly and have a level of decision-making autonomy. These individuals could also have outsized impact in the future as teams shift and agents take on more rote tasks.
|
It’s time to Think about Thoughtful Redesign |
Every industry and community will have to plan for what the AI future will bring. But there are a few reasons why the coming AI revolution will have such a strong impact in healthcare.
First, it's the single largest employer in America. The 22M strong workforce is distributed nationwide and is often one of the two largest employers in every American town. A rapid dislocation event has the potential to be broadly destabilizing, more than most other industries.
Second, every major efficiency created in healthcare to date has accreted to the bottom lines of industry players and never to lower prices for patients. We can’t watch a situation unfold where a plurality of every town's workers lose their jobs and, at the same time, the price of one of the few things they have to buy increases.
We all have a stake in the continued strength of our communities. In order for them to remain strong, we need to rally to a unifying agenda that supports American families through this transition, regardless of our political affiliation (the two authors of this piece are a registered Democrat and Republican). The good news is there’s endless jobs to be done in healthcare. Our task now is to make sure we have humans focused on the right ones.
|
Thanks to Chrissy and Mike for lending their voice to Hospitalogy:
- Mike Desjadon is CEO of Anomaly Insights and a member of the Virginia Board of Health. He has spent nearly two decades working across payer-provider dynamics, revenue cycle, and managed care, and previously held senior roles at Optum and The Advisory Board Company.
- Christina Farr is the CEO and editor-in-chief of Second Opinion Media and a GP at Scrub Capital. Second Opinion runs a regular newsletter on the business of healthcare, plus a podcast called Lifers about healthcare entrepreneurship. Previously she spent 15 years in venture capital and journalism. She’s also the author of an award winning book, “The Storyteller’s Advantage.”
|
|
|
|
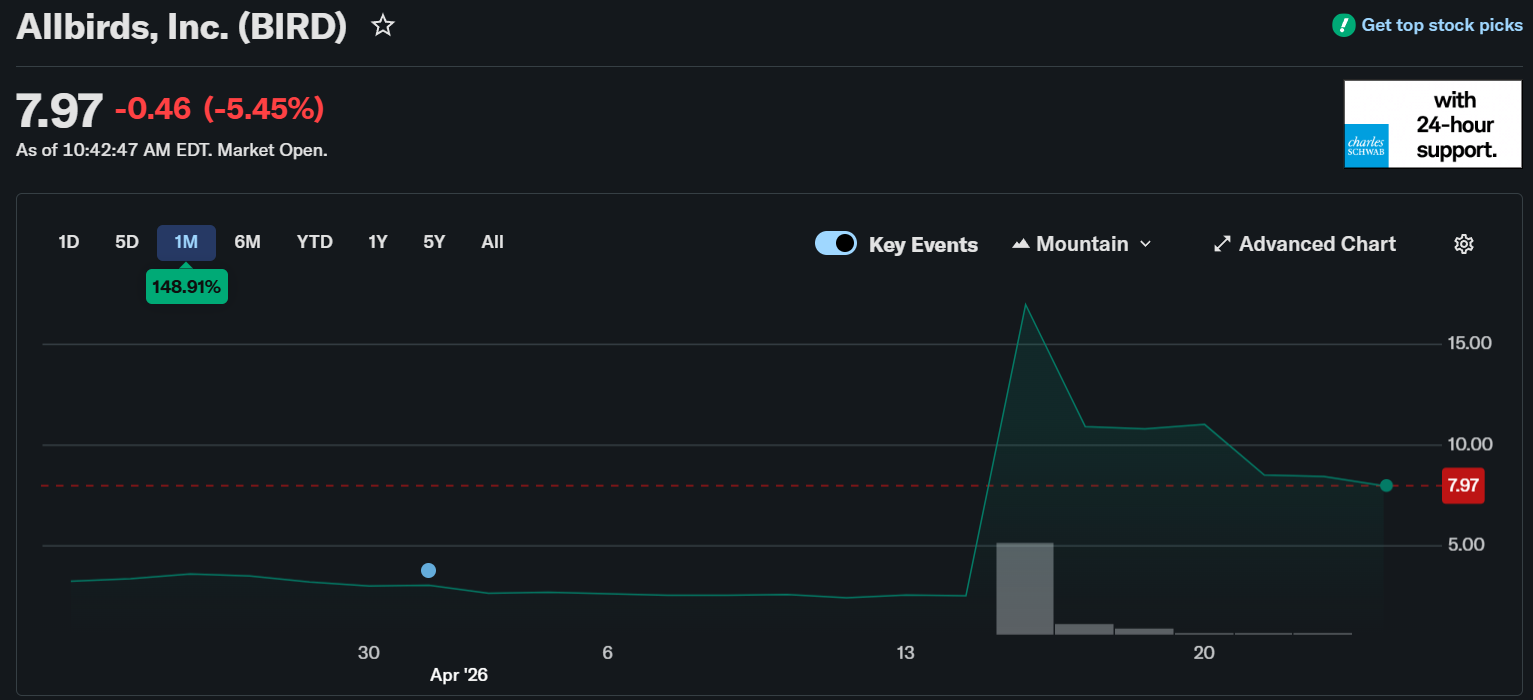
Allbirds…what in the world is happening here? In case you missed it, Allbirds has decided to go rogue as a company, ditching the fun millennial branding and going all-in on AI, becoming an AI infrastructure and data center company instead - now known as NewBird AI:
- NewBird AI expects to use initial capital from the Facility to acquire high-performance GPU assets, which will be deployed to serve customers requiring dedicated access to AI compute capacity. NewBird AI’s long-term vision is to become a fully integrated GPU-as-a-Service (GPUaaS) and AI-native cloud solutions provider. Over time, the Company intends to grow its neocloud platform by expanding its compute and service offerings, deepening partnerships with operators and customers, and evaluating strategic M&A opportunities.
Neocloud? What the hell are we even talking about here fam?
What’s crazier is that investors love the move as the stock is up 150% over the past month. And obviously this area has high demand and opportunity but…a pivot from a lovable shoe company into AI ‘neocloud’ infrastructure is not something I had on my bingo card.
|
It is the weirdest move I’ve seen since the crypto craze when some companies became meme stocks or said they were blockchain enabled or whatever, and it’s one of the biggest signals to me that we’re entering the end of the Goldilocks era in AI, and treacherously near bubble territory. While it’s impossible to time a bubble, there are always signs.
|
|
|
|
Thanks for the read! Let me know what you thought by replying back to this email.
— Blake
|
|
|
|
I'm building a community of leaders in strategy, finance, and ops
at hospitals and health systems to help us connect, learn, and grow together.
|
|
|
|
Get your brand in front of 68,400+ executives and healthcare decision-makers.
|
Workweek Media Inc.
1023 Springdale Road, STE 9E
Austin, TX 78721
Want to ruin my day? Unsubscribe.
|
|
|
|
|






No comments